How are the female pelvic organs located? The structure and physiology of the small pelvis of a woman

Topographic anatomy of the small pelvis.
Taz,pelvis.
Borders. The pelvis is a part of the body located between the abdomen and the lower limbs and bounded on the outside by the pelvic bones, the sacrum, the coccyx, and from below by the perineum.
External landmarks:
Iliac crest, crista iliaca; - superior anterior iliac spine, spina iliaca anterior superior; - pubic tubercle, tuberculum pubicum; - pubic symphysis, symphysis pubica; - dorsal surface of the sacrum, facies dorsalis os sacrum; - coccyx, os coccyges; - ischial tubercle, tuber ischiadicum; - greater skewer femur, trochanter major ossis femoralis; - subpubic angle, angulus subpubicus
Individual, sex and age differences:
1. Individual features of the pelvis. It consists in different ratios of the longitudinal and transverse diameters of the pelvic ring. With one extreme type of variability, the longitudinal diameter is larger than the transverse one, while the pelvis is “squeezed” from the sides, the axis pelvic organs more often inclined towards the sacrum. With another type of variability, the longitudinal diameter is less than the transverse one, the pelvis is “compressed” in the anteroposterior direction, and the axes of the pelvic organs are inclined towards the pubic symphysis.
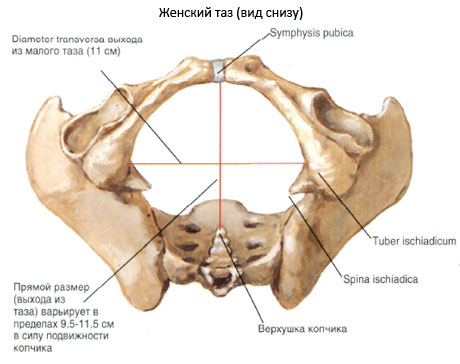
2. Sex differences in the pelvic skeleton: - wings ilium in women, they are located more horizontally, so in women the pelvis is wider and lower than in men; - the lower branches of the pubic bones in women are located at an obtuse angle and form a pubic arch, arcus pubis; in men, they are located at an acute angle and form a subpubic angle, angulus subpubicus;
The pelvic cavity in women has the shape of a curved cylinder, in men - a curved cone;
Pelvic tilt, inclination pelvis - the angle between the horizontal plane and the plane of the upper pelvic aperture - in women 55-60, in men 50-55.
3. Age differences. By the time of birth, the pelvis consists of 3 parts, each of which has ossification nuclei. All 3 parts - iliac, ischial and pubic - are connected by layers of cartilage in the acetabulum. The iliac fossa is almost absent. By the age of 7, the size of the pelvic bone doubles, then until the age of 12, growth slows down. By the age of 13-18, parts of the pelvic bone grow together, their ossification ends. The final synostosis of all elements of the pelvic bone is completed by the age of 25.
The walls of the pelvis. Limit the pubic, iliac, ischial bones, sacrum and coccyx.
pelvic floor form the pelvic diaphragm, diaphragma pelvis, and partly the urogenital diaphragm, diaphragma urogenitale.
urinary diaphragm,diaphragma urogenitale. It is formed by 2 muscles: the deep transverse muscle of the perineum and the external sphincter of the urethra.
D pelvic diaphragm. Formed by 2 muscles: the muscle that raises the anus, m. levator ani, and the coccygeal muscle, m. coccygeus.
Floors of the pelvic cavity. The pelvic cavity is divided into three floors: upper - peritoneal, cavum pelvis peritoneale, middle - subperitoneal, cavum pelvis subperitoneale, lower - subcutaneous, or perineal, cavum pelvis subcutaneum s. Perineale.
The course of the peritoneum in the male pelvis. Here the peritoneum passes from the anterior wall of the abdomen to bladder, covering the upper wall, partially - side and back. On the sides of the bladder, the peritoneum forms fossae paravesicales. At the level of the symphysis, the peritoneum forms the plica vesicalis transversa. Descending along the posterior wall of the bladder, the peritoneum covers the medial edges of the ampullae of the vas deferens, the tops of the seminal glands, and passes to the rectum, forming a rectovesical depression, excavatio rectovesicalis. Moreover, the supraampullary part of the rectum is covered with peritoneum on all sides, the ampulla is covered on 3 sides for a large extent, and Bottom part the rectum is not covered by the peritoneum at all.
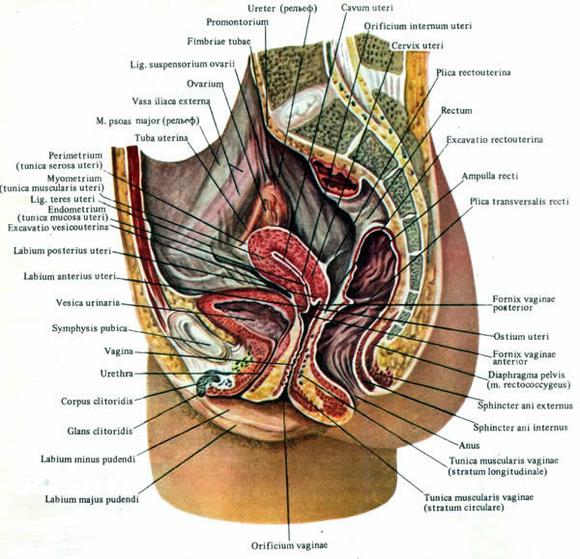
The course of the peritoneum in the female pelvis. Here the peritoneum also passes from the anterior wall of the abdomen to the bladder, forming a transverse fold, then covers its upper and posterior walls. After that, it passes to the anterior surface of the uterus at the level of its isthmus, forming a shallow vesicouterine cavity, excavatio vesicouterina. On the anterior surface of the uterus, the peritoneum covers only the body of the uterus. On the posterior surface of the uterus, the peritoneum covers the body, supravaginal part of the cervix and posterior fornix vagina and passes to the rectum, forming a deep recto-uterine cavity, excavatio rectouterina (Douglas space). It is limited by the folds of the peritoneum - plicae rectouterinae, which continue to the anterior surface of the sacrum.
Fascia and cellular spaces, their connections with cellular spaces of neighboring areas.
Parietal pelvic fascia, fascia pelvis parietalis, covers the back of the anterior surface of the sacrum and is called pre-sacral, fascia presacralis, on the sides - parietal muscles: m. piriformis, m. obturatorius internus, having the corresponding names (fascia obturatoria, fascia m. piriformis), in front - the posterior surface of the symphysis and the upper branches of the pubic bones, from below - the upper surface of m. levator ani.
Visceral pelvic fascia, fascia pelvis visceralis, lines the extraperitoneal parts of the pelvic organs in men and forms two sagittal spurs stretching from the pubic bones to the sacrum. Part of the visceral fascia, stretching from the pubic bone to the prostate gland in men or to the bladder in women, is called the pubic-prostatic, lig. Puboprostaticum, or pubic-cystic, lig. Pubovesicale, ligament. These ligaments accompany bundles of smooth muscle fibers m. Puboprostaticus and m.Pubovesicalis. The sagittal spurs of the visceral fascia, located behind the bladder, also contain bundles of smooth muscle fibers that form several muscles: rectococcygeal, m. sacrococcygeus; rectovesical, m. Rectovesicalis in men and recto-uterine in women. Lining the pelvic organs, the visceral fascia of the pelvis forms a capsule of the rectum (Amyusse capsule) and a capsule prostate(Pirogov-Reitzia capsule).
Cellular spaces. The main cellular spaces of the small pelvis are located within the subperitoneal floor of the pelvis.
Visceralcellular spaces are gaps between the wall of the organ and the visceral fascia. There are: paravesical, paraprostatic, paravaginal, paracervical and pararectal visceral cellular spaces.
Parietal cellular spaces in the subperitoneal floor of the small pelvis of a woman there are four: retropubic (pre-vesical). two lateral and presacral (posterior rectal). In men, one more, fifth , retrovesical cellular space.
Children's features.
The fasciae of the pelvis are very thin and loose. The parietal fascia is closely adjacent to the fascial sheaths of the parietal vessels. The parietal and near-organ cellular spaces contain a small amount of adipose tissue, which makes the anterior and
posterior Douglas space.
Internal iliac vessels.
The main arterial trunk that supplies blood to the pelvic organs is internaliliac artery, A. iliaca interna.
Branches of the internal iliac artery:
- parietal: A. ileolumbalis.,A. sacralis lateralis., A. obturatorius., A. glutea superior., A. glutea inferior.
- visceral :, A. umbilicalis (a. vasicalis superior)., A. vesicalis inferior., A. rectalis media., A. pudenda interna. A. uterina (a. ductus deferentis).
At the level of the upper edge of the greater sciatic foramen a. iliaca interna is divided into anterior and posterior trunks.
From the front trunk originate predominantly visceral arteries: aa. uterina, vesicalis inferior, rectalis media; two parietal arteries, aa. umbilicalis et obturatoria, are directed anteriorly. The umbilical artery has two parts: an open part, pars patens, from which the superior vesical artery and the artery of the vas deferens depart, and a closed part, pars occlusa. This obliterated part of the artery reaches the visceral fascia of the bladder and then, together with it, goes to the navel.
The end part of the anterior trunk at the piriform opening is divided into the internal genital, a. pudenda interna, and lower gluteal, a. glutea inferior, arteries.
Posterior trunk of the internal iliac artery gives off parietal arteries: aa sacrales laterales, iliolumbalis et glutea superior. A. iliolumbalis anastomoses with its lumbar and iliac branches with the lumbar and intercostal arteries and with a circumflexa ilium profunda and gluteal arteries. Due to this, collateral blood flow occurs when the common iliac artery is occluded.
Venous drainage from the pelvic organs carried out first in the venous plexus, which have the same names: pl. venosus rectalis, pl. venosus vesicalis, pl. venosus prostaticus, pl. venosus uterinus, pl. venosus vaginalis. Then the blood from these plexuses flows into internal iliac vein, which is located deeper than the artery and medial from it. The parietal veins accompany the arteries in the form of paired vessels.
Children's features.
The arteries of the small pelvis of a newborn have their own characteristics, due to the peculiarities of the blood supply to the fetus: the common iliac, internal iliac (its anterior trunk) and umbilical arteries are represented by a single main vessel the same diameter throughout.
The sacral plexus.
It is formed by the anterior branches of the IV and V lumbar and the anterior branches of the I, II, III, IV sacral spinal nerves exiting through the anterior sacral foramen. It lies on the anterior surface of the piriformis muscle.
From the sacral plexus depart short and long branches. short branches n. obturatorius is directed along the side wall of the pelvis to the obturator foramen. N. gluteus superior goes into the epipiriform opening with the same artery and vein. N. gluteus inferior and n. pudendus exit the pelvic cavity through the piriform opening. In addition, n. pudendus, internal arteries and the veins enter the ischiorectal fossa through the lesser sciatic foramen.
Together with them, they go into the gluteal region longbranches of the sacral plexus - n. ischiadicus and n.cutaneus femoris posterior and are sent to the piriform opening with the lower gluteal vessels.
Inferior hypogastric plexus, plexus hypogastricus inferior, - a vegetative plexus, including post-nodal sympathetic branches, parasympathetic nodes and sensory fibers for innervation of the pelvic organs. It descends in the form of a plate from the sacrum to the bladder.
Lymphatic vessels and regional lymph nodes.
Groups of lymph nodes: along the external and common iliac arteries (from the free lower limb; along the internal iliac artery (from the pelvic organs).; behind the rectal (from the sacrum, coccyx).
lymph outflow in the pelvis is carried out through three groups of nodes. The first is located along the internal iliac vessels: nodi iliaci interni. It collects lymph from the pelvic organs. The second group - nodi iliaci externi et communes, is located along the outer and common iliac arteries. They receive lymph from the lower limb, the lower parts of the abdominal wall, the superficial layers of the perineum, from the external genital organs. The third group - sacral nodes, nodi sacrales, collects lymph from the back wall of the pelvis and from the rectum. The nodes lying in the bifurcation of the common iliac arteries are called interiliac, nodi interiliaci. They receive lymph from both the pelvic organs and the lower limb.
Male pelvic organs.
Topography of the bladder.
The bladder is located in anterior section small pelvis, behind the pubic bones and symphysis, when filled, the bladder in an adult goes beyond the pelvic cavity, rising above the pubic bones. It distinguishes the top, body, bottom and neck. The wall of the bladder has well-defined muscular and submucosal layers. There are no folds and submucosal layer in the bottom of the bladder, the mucous membrane fuses with the muscular membrane. Here a triangular platform is formed, trigonum vesicae, or Lieta triangle. The peritoneum, passing from the anterior abdominal wall to the bladder, forms a transverse fold and covers a very small part of the anterior wall, upper and posterior walls. Passing from the back wall to the rectum, the peritoneum forms the vesico-rectal fold and the vesico-rectal recess, excavatio rectovesicale.
In the subperitoneal region, the bladder has a pronounced visceral fascia of its own. Between the wall of the bladder and the fascia in the perivesical space in a well-defined layer of loose fiber is the venous network of the bladder.
Syntopy of the bladder.
The anterior surface of the bladder, covered by the visceral fascia, is adjacent to upper branches pubic bones and pubic symphysis, separated from them by a layer of loose connective tissue of the retropubic (pre-vesical) cellular space. The ampullae of the vas deferens, the seminal glands, the terminal sections of the ureters and the fascia rectoprostatica (septum rectovesicale) are adjacent to the posterior surface of the bladder.
The vas deferens and the ureters crossing them from below and outside adjoin the lateral surfaces of the bladder for some length. From above and from the sides to the bladder, the loops of a thin, sigmoid, and sometimes transverse colon or caecum with a appendix separated from it by the peritoneum are adjacent. The bottom of the bladder is located on the prostate.
Bladder blood supply. It is carried out from the system a. iliaca interna. One or two a. vesicalis superior most often depart from the non-obliterated part of a. umbilicalis, a. vesicalis inferior - directly from the front trunk a. iliaca interna or from the obturator artery.
Bladder veins form a network in the visceral cellular space of the bladder. From there the blood is sent to venous plexus bladder and prostate, located in the retropubic space. Further, the blood flows into v. iliaca interna.
Lymph drainage from the bladder. It is carried out in nodi lymphoidei iliaci, located along the external iliac arteries and veins, and in nodi lymphoidei iliaci interni and sacrales.
Bladder innervation. The upper and lower hypogastric nerve plexuses, the pelvic splanchnic nerves and the pudendal nerve, which form on the walls of the bladder and especially at the confluence of the ureters and around them, the plexus vesicalis take part in the innervation of the bladder.
Children's features.
In newborns and young children, the topography of the pelvic organs is significantly different from that in adults. The bladder is mostly located above the symphysis, its anterior wall is not covered by the peritoneum and is adjacent to the anterior abdominal wall. The urinary duct runs from the upper wall of the bladder to the navel. The latter quickly becomes empty and obliterated, turning into a connective tissue cord. With the age of the child, an increase in the pelvic cavity occurs and the bladder, as it were, descends and, in an emptied state, is located in the cavity of the small pelvis behind the pubic joint.
Topography of the ureters.
The ureter is a paired organ, along its length it has 3 narrowings: at the beginning of the ureter, at the place where the abdominal part of the ureter passes into the pelvic part, and at the place where it flows into the bladder.
The pelvic section of the ureter, which is approximately half of its length, starts from the border line of the pelvis. At the level of this line, the left ureter crosses the common iliac artery, and the right ureter crosses the external iliac artery.
Further, the ureter is located on the side wall of the pelvis in the lateral cellular space medially from the nerve trunks and internal iliac vessels of the pelvis and laterally from the rectum. Then the ureter crosses the obturator neurovascular bundle and the beginning of the umbilical artery and goes medially to the bottom of the bladder.
Here the ureter passes between the posterior wall of the bladder and the anterolateral wall of the ampulla of the rectum and crosses at right angles to the ductus deferens, located outward from it and anterior to the seminal glands.
blood supply the pelvic ureters is carried out from aa. rectales mediae and aa. vesicales inferiores.
Deoxygenated blood flows into vv. testiculares and vv. iliacae internae.
Pelvic ureters innervated from the upper and lower hypogastric plexuses, and in the lower part they receive parasympathetic innervation from nn. splanchnici pelvini.
lymph outflow from the pelvic ureters occurs in the iliac lymph nodes.
Topography of the prostate.
The prostate consists of 30-50 glands, forming substantia glandularis, and a muscular substance, substantia muscularis, representing the stroma of the gland. The glands through the ductuli prostatici open into the prostatic part of the urethra. The prostate is located in the subperitoneal floor of the small pelvis. It has a cone-shaped shape and is directed downward, towards the urogenital diaphragm. The base of the prostate is located under the bottom of the bladder. The prostate has two lobes and an isthmus. The prostate has a visceral fascial capsule, capsula prostatica (Pirogov-Retzia), from which mm go to the pubic bones. (ligg.) puboprostatica.
Syntopy of the prostate.
Above the prostate are the bottom of the bladder, the seminal glands and the ampullae of the vas deferens. Below is the urogenital diaphragm, in front is the posterior surface of the pubic symphysis, behind is the Denonville-Salishchev fascia rectoprostatica and the ampulla of the rectum. The prostate is easy to feel through the rectum.
Blood supply to the prostate carried out by branches from aa. vesicales inferiores and aa. rectales mediae (from a. iliaca interna). Vienna form a venous plexus, plexus prostaticus, which merges with the plexus vesicalis; further blood flows into v. iliaca interna.
innervation carry out branches of the lower hypogastric plexus.
lymph outflow from the prostate is carried out in The lymph nodes located along a. iliaca interna, a. iliaca externa and on the pelvic surface of the sacrum.
Topography of the vas deferens.
The pelvic section of the vas deferens is located in the subperitoneal floor of the small pelvis, divided into parietal, intermediate, and cystic. This part is located in the retrovesical cellular space.
Coming out of the deep inguinal ring, the vas deferens, first accompanied by the artery of the same name, and then leaving it, goes around from outside to inside and down a. epigastric inferior. Rounding a. et v. iliacae externae, the vas deferens is directed medially and backwards into the lateral space of the pelvis. Here it crosses the obturator neurovascular bundle, the umbilical artery, and the superior cystic arteries.
Located medially from these vessels, the vas deferens reaches the side wall of the bladder, then passes between the ureter and the posterior surface of the bladder, forming the ampulla of the vas deferens, ampulla ductus deferentis. On the back wall of the bladder, the ampoule is located medially from the ureter and seminal gland.
The duct of the ampoule, merging with the duct of the seminal gland, ductus excretorius, forms the ejaculatory duct, ductus ejaculatorius, which penetrates the prostate and opens to seed tubercle into the prostate urethra. The vas deferens are supplied with blood from a. ductus deferentis.
Topography of the seminal glands.
They are saccular protrusions outside of the terminal sections of the ductus deferens. They are surrounded by the visceral fascia and are located between the posterior wall of the bladder and the anterior wall of the ampulla recti.
Syntopy of the seminal glands.
Anterior to the glands are back wall bladder and terminal ureters. Medially, they are adjacent to the vas deferens with ampullae. The lower sections of the glands lie at the base of the prostate, and the superomedial sections are covered by the peritoneum, through which they come into contact with the intestinal loops.
blood supply seminal glands is carried out by aa. vesicalis inferior et rectalis media. The veins drain into the plexus vesicalis.
Innervated inferior hypogastric plexuses.
Lymph drainage from the seminal glands goes through the lymphatic vessels of the bladder to the lymph nodes located along the iliac arteries and on the sacrum.
Children's features.
In boys, the prostate gland and seminal vesicles are also located relatively high compared to their position in adults.
Topography of the rectum.
The rectum (rectum) is a continuation of the sigmoid colon and is located within the small pelvis at the anterior surface of the sacrum.
The rectum ends at the level of the pelvic diaphragm (m. levator ani), where it passes into the canalis analis. The length of the rectum is 10-12 cm.
In the rectum, the supraampullary part and the ampulla are isolated. supraampullary part and upper half ampoules are located in the upper, peritoneal floor of the small pelvis. The lower half of the ampulla of the rectum is located in the subperitoneal floor of the pelvis and instead of the peritoneum is covered with visceral fascia (Amyusse capsule).
The pelvic part of the rectum, in accordance with the curvature of the sacrum and coccyx, forms a bend directed backward by a bulge, nexura sacralis. At the transition to canalis analis, the final section of the rectum deviates downward and backward, forming a second bend, anal-rectal, flexura anorectalis (flexura perinealis), facing forward with a bulge.
The rectum makes three bends in the frontal plane. These include the upper right lateral bend, flexura superodextra lateralis, the intermediate left lateral bend, flexura intermediosinistra lateralis, the lower right lateral bend, flexura inferodextra lateralis.
Layers of the rectum- muscular membrane (consists of the outer longitudinal, stratum longitudinale, and the inner circular, stratum circulare, layers).
At the level of the pelvic diaphragm above the fibers of the external sphincter, m. sphincter ani externus, m fibers are woven into the muscles of the rectum. levator ani, in particular m. puboanalis, etc. puborectalis.
mucous membrane upper division ampulla of the rectum forms 2-4 transverse folds that do not disappear when the rectum is filled, plicae transversae
recti, having a helical course. In the ampullar part, there is one fold on the right wall, two on the left.
Syntopy of the rectum.
In the subperitoneal floor anterior to the rectum are the posterior wall of the bladder not covered by the peritoneum, the prostate, the ampullae of the vas deferens, the seminal glands (vesicles) and the terminal sections of the ureters. The rectum is separated from them by Denonville-Salishchev's fascia rectoprostatica (septum rectovesicale). On the sides of the ampulla are the branches of the internal iliac vessels and the nerves of the plexus hypogastricus inferior. Behind the rectum adjoins the sacrum. .
Blood supply: a. rectalis superior (unpaired - terminal branch of the lower mesenteric artery) and a. rectalis media (steam room, from a. iliaca interna). .
Venous return: veins form a venous plexus, plexus venosus rectalis, in the wall of the rectum, in which the submucosal and subfascial parts are isolated. From the upper sections, the blood flows through v. rectalis superior, which is the beginning of v. mesenterica inferior (portal vein system). All veins anastomose widely among themselves and with the veins of other pelvic organs. Thus, there is one of the portocaval anastomoses here.
In innervation the lower mesenteric, upper and lower hypogastric plexus and pelvic splanchnic nerves take part. As part of the sacral spinal nerves are sensory nerves that convey the feeling of filling the rectum.
lymph outflow from the nadampular part of the rectum and partly from the upper part of the ampulla through the nodi pararectales along the superior rectal artery to the nodi rectales superiores and further to the nodi mesenterici inferiores. This explains the possibility of spread of cancer metastases along the rectum. From the subperitoneal region of the rectum, lymph flows to the internal iliac and sacral lymph nodes.
Children's features.
The rectum in newborns is located high, expanded and its curves are weakly expressed. It is adjacent to the ureters, bladder and vagina (in girls), prostate and seminal vesicles (in boys). With the growth and development of the child, the topographic and anatomical relations of the rectum approach those in adults.
Organs of the female pelvis.
Topography of the bladder in women.
The bladder in the female pelvis lies deeper in the pelvic cavity than in men. In the peritoneal floor, behind the bladder of women, the body of the uterus and loops of the intestine, which enter the excavatio vesicouterine, are adjacent. In the subperitoneal floor, the bladder adjoins the pubic symphysis with its front surface and is fixed to it by the pubic-vesical muscles (ligaments), mm. (ligg.) pubovesicalia. The back wall of the bladder lies anterior to the cervix and vagina. The bubble is firmly connected with the vagina, separating from it only with an insignificant layer of fiber, with the uterus the union is more loose. The bottom of the bladder is located on the urogenital diaphragm. Laterally adjacent to it m. levator ani.
At the bottom of the bladder in women, in front of the anterior wall of the vagina, the ureters flow into it.
The lymphatic vessels of the bladder in women are connected with the lymphatic vessels of the uterus and vagina at the base of the broad ligament of the uterus.
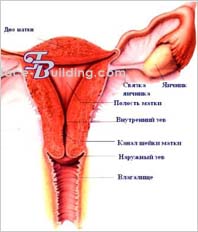
Topography of the uterus and its appendages.
The uterus is located in the small pelvis between the bladder in front and the rectum in the back. It consists of two sections: the upper one - the body, corpus, and the bottom, fundus, and the lower one - the cervix, cervix uteri. In the neck, supravaginal and vaginal parts, portio supravaginalis and portio vaginalis are distinguished.
On portio vaginalis cervicis there is an opening of the uterus, ostium uteri, limited in front of labium anterius and behind labium posterius. This hole connects the vagina through the canalis cervicis uteri with the uterine cavity, cavum uteri. The lateral edges of the uterus are called margo uteri dexter et sinister. For the most part, the uterus is located in the upper, peritoneal, floor of the small pelvis.
Suspension apparatus uterus. Formed by round and wide ligaments of the uterus, ligg. teres uteri and ligg. lata uteri. The broad ligaments of the uterus are a duplication of the peritoneum. They depart from the uterus almost in the frontal plane and reach the peritoneum of the side walls of the pelvis. In this place, the peritoneal sheets of the broad ligament form the suspensory ligament of the ovary, lig. suspensorium ovarii, containing the vessels of the ovary (a. et v. ovarica). Down and back from the angle of the uterus in the thickness of the broad ligament departs own bundle ovary, lig. ovarii proprium. Down and anteriorly from the angle of the uterus, the round ligament of the uterus, lig. teres uteri.
The uterus has a visceral fascia. Muscular fibrous bundles of the main ligament of the uterus, lig. cardinale. Ligaments attached to the visceral fascia: cardinal ligaments, ligg. cardinalia, recto-uterine, ligg. rectouterina, pubocervical. ligg. pubocervicale
The pubic-vaginal muscle, m. Pubovaginalis; urethrovaginal sphincter, m. sphincter urethrovaginalis and perineal membrane, membrana perinei.
blood supply carried out by two uterine arteries, aa. Uterinae, ovarian arteries, aa. ovaricae (from abdominal aorta), and the arteries of the round ligament of the uterus, aa. lig. teretis uteri. A. Uterina is a branch of the internal iliac artery. Venous outflow from the uterus occurs first in the uterine venous plexus, plexus venosus uterinus. It widely anastomoses with all the veins of the pelvis, but primarily with the venous plexus of the vagina, plexus venosus vaginalis. From the plexus, blood flows through the uterine veins into the internal iliac veins.
Outflow from the bottom of the uterus, ovaries and tubes occurs in the inferior vena cava through vv. ovaricae.
Innervation of the uterus carried out by an extensive uterovaginal nerve plexus, plexus uterovaginalis - the middle section of the paired lower hypogastric plexus, plexus hypogastricus inferior.
lymph outflow from the uterus from the visceral parauterine and paravaginal nodes (nodi parauterini et paravaginales), the lymph flows into the iliac lymph nodes and further into the common iliac nodes. Along the way ligg. cardinalia from the cervix, lymphatic vessels carry lymph to the obturator lymph nodes, and then to the external and common iliac nodes. From the bottom of the uterus along the outlet lymphatic vessels the round ligament of the uterus, the lymph partially flows to the inguinal lymph nodes.
The fallopian tubes.
The fallopian tube, tuba uterina, or fallopian tube is a paired organ that connects the uterine cavity with the peritoneal cavity. It is located along the upper edge of the broad ligament of the uterus and has a mesentery, mesosalpinx, which is part of the broad ligament just below the tube.
Diameter fallopian tube varies and ranges from 5 to 10 mm. In the tube, the uterine part, pars uterina, with the uterine opening, ostium uterinum, isthmus, isthmus, ampulla, ampulla, and funnel, infundibulum are distinguished. The funnel of the fallopian tube has fringes, fimbriae, bordering the abdominal opening of the tube, ostium abdominale tubae uterinae. One of the fimbriae, approaching the tubal end of the ovary, is called fimbria ovarica.
blood supply The fallopian tubes originate from the ovarian and uterine arteries
Ovaries. Ovary - women's steam room gonad measuring 1.5 x 1.5 x 1.0 cm. It is covered with germinal epithelium. The transition of the epithelium into the endothelium of the peritoneum is marked with a whitish line. In this place, the mesentery of the ovary ends, mesovarium, extending from the posterior leaf of the broad ligament of the uterus.
The ovary has two ends - tubal and uterine, two surfaces - medial and lateral, two edges - free and mesenteric. The ovary is attached to the posterior surface of the broad ligament of the uterus near the side wall of the pelvis. Under the peritoneal cover, a. approaches the ovary. ovarica from the retroperitoneal space. The uterine end of the ovary is connected with the body of the uterus through the connective tissue of the ovary's own ligament, lig. ovarii proprium.
blood supply ovary is carried out by a. ovarica, extending from the abdominal part of the aorta at the level of the 1st lumbar vertebra, as well as the ovarian branch of the uterine artery.
Outflow of venous blood from the ovary occurs through v. ovarica dextra directly into the inferior vena cava, through v. ovarica sinistra - first to the left renal vein and through it into the lower hollow.
In innervation ovary involved branches of the lower hypogastric plexus.
Lymph drainage from the ovary is carried out along the efferent lymphatic vessels accompanying the ovarian artery, to the lymph nodes located around the aorta, and to the iliac lymph nodes.
Children's features.
In newborn girls, the uterus is located above the plane of entry into the small pelvis. She has not finished her development and her body is 1/3, and the cervix is 2/3 of the entire length.
The ovaries are located near the boundary line of the pelvis. With age, the uterus and ovaries descend, and by the age of 12-14 they occupy a position corresponding to their position in women. By this age, the size of the uterus increases and the length of its body and cervix becomes the same.
Topography of the rectum in women.
The structure, division into sections, blood supply and innervation of the rectum in women do not differ from those in men. Only the syntopy and lymph drainage of the rectum in women differ.
In the peritoneal floor anterior to the rectum in women, the body, cervix and posterior fornix of the vagina are located. Between the rectum and the posterior wall of the body of the uterus there are loops descending from the lower floor of the abdominal cavity small intestine. They enter the recto-uterine cavity, excavatio rectouterina. In the subperitoneal floor, the rectum in women is adjacent to the vagina in front. However, they are separated by the fascia rectovaginalis. This fascia is rather thin and loose, it is penetrated by lymphatic vessels, so that it does not become an obstacle either to the spread of metastases in tumors of both organs, or to the development of rectovaginal fistulas.
Malformations genitourinary system in children.
Cysts of the urinary duct (urachus). They are formed with incomplete obliteration and sometimes have a fistulous tract that opens in the navel area - vesico-umbilical fistulas. Also to congenital fistulas includes vesico-intestinal fistulas, which are extremely rare. They usually occur between the rectum and the area of the bladder triangle, sometimes combined with atresia. anus.
In addition, in girls, ectopic laying of endometrial elements can occur in the urinary duct. In these cases, during puberty during the menstrual period, cysts filled with blood can form in the cord left from the urinary duct. In the presence of a fistulous tract, blood may be released from the navel.
Bladder exstrophy. This malformation is characterized by the absence of the anterior wall of the bladder and part of the anterior abdominal wall. The bladder is open anteriorly, the mucosa, according to the defect of the bladder wall, is fused with the edges of the skin defect. Pinholes of the ureters are clearly visible on the posterior wall of the bladder mucosa. Urine continuously flows out of them.
Hypospadias is a malformation characterized by the absence of part of the lower wall of the urethra.
Epispadias - underdevelopment of the upper wall of the urethra.
Malformations of the rectum.
Atresia of the anus, atresia ani. With this defect, there is no anus and the rectum ends blindly close to the skin of the perineum. The bowel is usually distended with accumulated meconium.
With atresia of the rectum, atresia recti, the anus is represented by a pronounced depression, but the rectum is short and blindly ends above the bottom of the small pelvis. In this case, the blind end of the rectum is separated from the perineum by a significant layer of tissue.
With atresia of the anus and rectum, atresia ani et recti, which occurs more often than other malformations, the anus remains closed, and the rectum ends blindly at different distances from the pelvic floor.
Topography of the perineum.
Borders, areas.
Perineum (region perinealis), forming the lower wall of the pelvic cavity, has the shape of a rhombus and is limited in front by the pubic symphysis, in front and laterally by the lower branch of the pubis and the branch of the ischium, laterally by the ischial tuberosities, laterally and posteriorly by the sacrotuberous ligaments, and posteriorly by the coccyx. A line connecting the ischial tuberosities (linea biischiadica) . the perineum is divided into the urogenital and anal regions. The tendon center of the perineum is usually projected into the middle of the line connecting the ischial tubercles.
Layers of regions and their characteristics.
The layered structure of the anal area in men and women is almost the same. In the center of the anal region is the anal opening of the direct kateshka, anus.
1 .Leather(derma) at the anus it is pigmented, thinner than along the periphery of the region, and fused with the subcutaneous part of the external sphincter of the anus, as a result of which it forms folds, and then passes into the mucous membrane of the rectum. In men, between the root of the scrotum and the anus is the perineal suture, raphe perinei.
2. Subcutaneous adipose tissue And superficialfascia of the anal area (panniculusadiposusfascia perinei superficialis) better expressed than the genitourinary. In the fiber are the skin branches of the lower gluteal and lower rectal arteries and the subcutaneous venous network, which is especially thickened near the anus. Innervate the skin of the branch nn. rectales inferiores from n. pudendus in the medial parts of the region and rr. perineales from n. cutaneus femoris posterior in the lateral sections.
Where are the muscles pelvic floor womenConsider the structure of the female pelvic organs, after all, it is the muscles of the small pelvis that we are going to strengthen with Kegel exercises, gymnastics for intimate muscles, training methods - wumbling / imbilding / intimate fitness, as well as with the help of popular vaginal simulators Jade Egg and KEGEL BALLS recommended for self-development. |
The uterus, bladder, rectum have a separate entrance (sphincter). The sphincters pass through the muscles of the pelvic floor. The pelvic organs have very elastic muscles that can contract and stretch strongly.
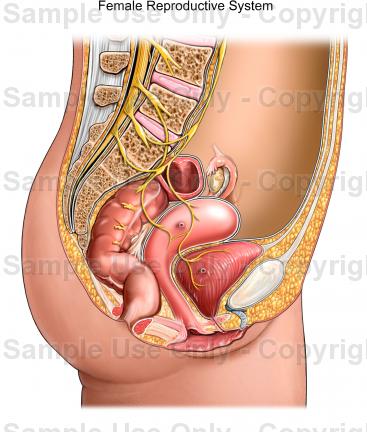
Female pelvic organs fit snugly enough to each other and are in a curved position. In this case, the uterus rests on the bladder, the bladder - on the vagina. The rectum is supported by the coccyx. This position ensures the stability and proper functioning of the pelvic organs. Especially such support is required in a standing position. If the correct position of one of the pelvic organs is violated, the entire interconnected system is disrupted, causing diseases of the pelvic organs.
Pelvic muscles hold everything securely pelvic organs inside to anatomically correct position. Stretched like a hammock from below the pelvis, muscle layer(pubic-coccygeal muscle) consists of internal and outer layers muscles that work together to hold and normal functioning pelvic organs, and therefore women Health. Along with developing and strengthening the muscles of the small pelvis, Kegel exercises also increase blood flow to the pelvic area which stimulates enhanced cell renewal.
Like other muscles pelvic muscles can only be kept in good shape through regular exercise.
Weakened muscles of the perineum and pelvis can lead to such unpleasant manifestations as urinary or fecal incontinence, due to insufficient self-control of the functioning of the intestines or bladder.
Weak pelvic muscles can also lead to difficult labor due to insufficient muscle activity during labor activity, decrease sexual desire and satisfaction from intimacy, prolapse of the uterus and vagina, and even prolapse internal organs cause many dysfunctions and diseases of the pelvic organs.
Muscles of the vagina
The vagina is an elastic canal, an easily stretchable muscular tube that connects the vulva and uterus. The average length (depth) of the vagina is between 7 and 12 cm. The size of the vaginal canal for each woman may vary slightly.
The walls of the vaginal muscle consist of three layers: inner, middle (muscular) and outer.
|
Muscles of the vagina are made up of smooth muscle. The muscle bundles are oriented mainly in the longitudinal direction, but there are also circular bundles. In the upper part of the vaginal muscles pass into the muscles of the body of the uterus. In the lower part of the vagina, the muscles become stronger, gradually weaving into the muscles of the perineum. The muscles of the vagina, like any smooth muscle, cannot be controlled consciously, but at the same time, the muscles of the vagina can be greatly stretched during labor. You can control the compression of the muscles of the vaginal canal by changing the intra-abdominal pressure, increasing its strength, we get compression, and decreasing it, relaxation. |
 |
Intra-abdominal pressure is created in abdominal cavity, which is limited from below by the muscles of the pelvic floor, from above by the respiratory diaphragm, in front and sides - by the transverse muscles of the press, behind - by the muscles of the back.
If you simultaneously strain the muscles of the pelvic floor, lower the respiratory diaphragm and retract the abdominal muscles, then intra-abdominal pressure increases and the walls of the vaginal canal (vagina) are compressed.
The vaginal compression technique is mainly used during intimacy, for stronger compression of the partner's penis along the entire length of the vagina, or to massage the walls of the vaginal canal.
How to strengthen your pelvic floor muscles
For the development of the pelvic floor muscles and the ability to control them, use Kegel exercises, gymnastics for intimate muscles, wumbilding / imbilding and similar techniques.
To develop a skill management intra-abdominal pressure use pneumatic vaginal simulators.
Similar content
Kegel exercises for women - Help with uterine prolapse, urinary incontinence
Kegel gymnastics for the pelvic floor muscles - A set of exercises according to the Kegel method
Step-by-step instructions for performing exercises with the KEGEL BALLS simulator - A technique for independent development. Alternatively, the Jade Egg trainer can be used. Attention! Perform only after preliminary strengthening of the pelvic muscles with the help of exercise without equipment.
|
Any woman at least once in her life - or even more - faced pain and other unpleasant sensations lower abdomen. In this regard, many are interested in what is included in the concept of "pelvic organs" in women, what organs and their systems.
Bladder
In the pelvis of a woman, like a man, the bladder is located. This is a single muscular organ, which collects and accumulates urine flowing from the kidneys. Attached to the bottom of the bladder are the so-called urinary tract, which are actually represented by just one hollow tube ( urethra) through which urine is excreted from the body.
The bladder is located in a woman behind the pubis. It is medium in size and in shape resembles a turnip tapering downwards. This organ can hold up to 700 ml of fluid. When it is completely filled, it enters the brain nerve impulse which causes the urge to urinate.
Rectum
The rectum is another organ located in the small pelvis. She is the most lower section intestines and all digestive system. The rectum has an oblong shape, similar to a large ampulla. Its length may vary, but on average it is 15-16 cm.
The rectum ends with a sphincter (pulp), which closes the lumen into it and keeps the excrement inside it. There they accumulate a certain moment until a person again has a desire to go to the toilet (the brain is also responsible for the work of these impulses).
reproductive organs
Women's
In women, the uterus is located in the pelvis. It is a single organ, consisting of almost the same muscles. The uterus in its shape is somewhat reminiscent of a pear, turned with a narrow end down. On both sides, the fallopian tubes are attached to the uterus, at the ends of which the ovaries are located. Both the ovaries and the tubes are the paired organs of the woman's small pelvis.
The ovaries have a special, cortical layer. It contains a large number of tiny eggs, each of which is located in the so-called follicle. When 1 such follicle matures, the egg comes out and enters the fallopian tube. On it, she moves towards the uterus. If on its way the egg meets a sperm cell and it penetrates inside it, then fertilization occurs.
At the bottom, a long hollow "pipe" is attached to the uterus. This is the vagina. Its length is on average 10 cm. The lower end of the vagina is connected to the external genital organs. The vagina during labor is birth canal. During sexual intercourse, it serves as the site of entry of the male genital organ.
Men's
In men, the prostate gland is located primarily in the pelvis. It consists of muscular-glandular tissue and is located in men at the very bottom of the bladder. It produces a special liquid, which is called a secret and is part of the sperm. Seminal vesicles (2 pieces) are also located in the pelvis. They are involved in the process of sperm production and ejaculation.
In general, all organs of the small pelvis are an important distinguishing feature, which has the anatomy of a woman. It represents the bone part of the birth canal, the small pelvis of a woman.
The sphincters pass through the muscles of the pelvic floor. The pelvic organs have very elastic muscles that can contract and stretch strongly.
Female pelvic organs
In this case, the uterus rests on the bladder, the bladder - on the vagina. Along with the development and strengthening of the muscles of the small pelvis, Kegel exercises also increase blood flow to the pelvic region, which stimulates enhanced cell renewal. Perform only after preliminary strengthening of the pelvic muscles with the help of exercises without simulators.

In this article, we will try to explain how the basis of this frame is arranged in the body of a woman. The structure of the female pelvis is due to the main physiological function women - bearing and giving birth to healthy offspring.
Ultimately, human female pelvis its structure is absolutely unique. The female pelvis is larger than the male, wider and more flattened from above. The cavity of the male small pelvis is similar in shape to a card suit of hearts, and the cavity of the female round shape. The female sacrum is wider and less concave.

The basis of the bone skeleton of the pelvis are two pelvic bones, sacral and coccygeal sections of the spine, interconnected by a ring.
The structure of the female pelvis
The muscles of the pelvis are divided into external, middle and internal. TO internal muscles of the small pelvis also include: the muscle that lifts the anus, the coccygeal muscle, the sphincter of the anus. The middle muscles of the small pelvis are represented by the urogenital diaphragm, which consists of the deep perineal muscles and the external urethral sphincter.
Anatomy of the pelvis of a woman
The muscles of the small pelvis are powerful, well developed, richly supplied with blood. In the center of the small pelvis is the uterus, in front of it is the bladder, behind the rectum. The uterus consists of three sections: fundus, body and cervix. The uterus is covered with peritoneum from the front to the neck.
Blood supply of the small pelvis. The blood supply to the pelvic organs of a woman is provided by vessels branching off from the abdominal artery by the common iliac arteries. As a result, from the internal iliac arteries branch following vessels small pelvis: uterine, middle rectal, internal pudendal, superior cystic artery.

In this article, we will consider the structure of the pelvic organs of a woman, give a diagram and talk about possible anomalies in this area.
Next, we will talk about the features female structure small pelvis and about those organs that are familiar only to the beautiful half of humanity. Uterine fibroids, in contrast, are usually found in menopausal women.
https://youtu.be/VAjdjcyUGkU
Both pelvic bones, connecting with each other and with the sacrum, form a bone ring of the pelvis, pelvis, which serves to connect the trunk with the free lower limbs.
On the sides, the walls of the small pelvis are formed by sections of the pelvic bones corresponding to the acetabulum, as well as sit bones along with the ligaments going to them from the sacrum. Pelvic measurements by obstetricians are made using a compass.

In Neanderthals, the pelvis has all human features, which indicates vertical position body and bipedal walking, but it is still somewhat narrower than that of a modern person.
The wings of the ilium in women are more deployed to the sides, as a result of which the distance between the spines and crests is greater than in men. The entrance to the female pelvis has a transverse-oval shape, while the shape of the entrance to the male pelvis is rather longitudinal-oval.
The pelvic inlet in men is much narrower than in women; in the latter, the ischial tuberosities are further apart and the coccyx protrudes less forward.
Pelvic muscles
The pelvic cavity in men has a clearly expressed funnel shape, in women this funnel shape is less noticeable and their pelvic cavity approaches a cylinder in outline.
The basis of the pelvis is formed by two pelvic bones, the sacrum and the coccyx, connected by the joints of the belt lower extremities into a bone ring, inside which a cavity is formed that encloses the internal organs.

The size and shape of the pelvis are importance For birth process and are to be measured and evaluated in all pregnant women. To determine the size of the pelvis, a measuring instrument is used - Martin's pelvis, as well as manual examination through the vagina.
Anatomy of a woman. Human Anatomy (Biology, Grade 8)
That is why human anatomy has been studied since school. Before that, the guys have already considered the structure of plants and animals, so it will be easier for them to learn an anatomy lesson, despite the complex, multifaceted material on the structure of a person.
Possible anomalies in the development of the pelvic organs in women
So, for example, almost at the end of the school year, when children have become even older and can adequately perceive material of a corresponding nature, the anatomy of a woman and a man begins to be studied.

Which doctors to contact for a pelvic exam:
The anatomy of a woman is an important and complex issue, enough intimate nature. Pair formations in female body, having an outer and inner part. The first is a skin-covered organ various shapes(round, pear-shaped, elongated, and so on).
Where are the pelvic floor muscles located?
This area has a different coloration, which depends on the race of the woman and whether she was in labor.
What diseases are associated with the pelvis:
The main difference between male and female anatomy, of course, not only in the absence or presence of mammary glands. In fact important role plays the structure of the small pelvis and its organs. In general, not only a small, but also a large pelvis is distinguished. It is located immediately above the first.
The pelvic cavity is formed by a wide and narrow part. The anatomy of a woman presupposes, first of all, the presence of obvious external differences By gender. The anatomy of a pregnant woman changes significantly. The anterior wall of the small pelvis is presented pubic bones and symphysis, the lateral ones are formed by the ischial bones, and the back wall consists of the sacrum and coccyx.
In the structure of the pelvis in an adult, sexual characteristics are clearly visible: the female pelvis is wider and flattened than in men, the pelvic cavity in women is also larger.
