After bowel resection. Indications and technique for small bowel resection Small bowel resection with anastomosis
Small bowel resection is preferred over small bowel bypass in situations where the neoplasm is limited to the small bowel and is not associated with pelvic structures, especially after irradiation and with abundant adhesions, or where a loop of the small bowel is involved in a pelvic tumor. Bypass resection should also be performed in cases where extensive small bowel resection is not required to locate and mobilize the pathologic segment. If the surgeon is forced, due to the extent of the lesion, to mobilize and remove the entire small intestine, resection of the ileum and sigmoid colon is required, and a high ileograft colostomy is required.
Multiple enterotomies not only increase the risk of intestinal contents entering the wound, but are often overlooked during the operation. In addition, enterotomies that are subsequently repaired form multiple adhesions to the pelvic wall and recurring intestinal skin and/or vaginal fistulas may form at the suture line. Thus, experienced pelvic surgeons have come to the difficult conclusion that small bowel resection should be performed in those few cases where the pathological segment of the small bowel can be easily mobilized and isolated. Otherwise, a small bowel bypass should be performed.
The pathological segment of the small intestine is removed, and the remaining small intestine is re-tightened to a healthy segment of the intestine.
Physiological changes
Removal of large segments of the small intestine can lead to postoperative diarrhea and reduced absorption of fat-soluble vitamins.
Attention!
The main focus of attention during resection of the small intestine should be directed to ensuring the vascular integrity of the anastomosis. Vascularization of a 10 cm area of the small intestine is unreliable. In patients after intense irradiation, it is preferable to perform an ileoscopic colostomy rather than an ileostomy for anastomosis at a 10 cm ileum.
The advantage of a shallow outline of the small intestine is that it avoids extensive dissection in a heavily irradiated pelvic space with abundant adhesions. Only the dissection needed to perform the bypass should be made, and the remainder of the affected bowel should be removed if the pelvic organs have been heavily irradiated. Both resection and bypass procedures are required early in pelvic surgery, however, both are illustrated in this section.
Execution technique
Shown here is a small bowel resection using a penetrating anastomosis using the Gambee technique. Creating an anastomosis using a surgical stapler is shown on the example of the bladder and ureter with an intestinal loop.

1 - Patients for resection of the small intestine are placed in the supine position. A Foley catheter is inserted into the bladder. A nasogastric tube is passed into the stomach.

2 - Before the operation, a thorough bilateral examination is carried out.

3 A median incision is made, usually around the umbilicus. After laparotomy, the abdominal cavity is examined. As mentioned above, in most cases, small bowel disease associated with pelvic disorders is within one meter of the ileocecal angle. This fact is of great importance to the pelvic surgeon as it allows the surgeon to trace the small intestine from the caecum, rather than separating the intestine from the tricetal ligament. At this stage, a decision must be made to either perform a bowel resection or to bypass the small intestine. If the extent of the small bowel lesion is visible and there is a possibility of mobilization without extensive dissection, small bowel resection becomes the procedure of choice. If, as happens in most cases, the diseased segment of the small intestine is embedded deep into the small pelvis, especially after intense irradiation, it is more reasonable to perform a local bypass of the intestine.nbsp;

4 - The small intestine to be resected is mobilized, and the mesentery is carefully examined to isolate the vascular arcades. The point of transection is chosen far enough from the affected part and in close proximity to the healthy vascular arcade. The bowel should be fixed between Babcock clamps or warm gauze soaked in saline held between the thumb and first finger. The peritoneum on the mesentery is opened with a scalpel, using a technique that avoids crossing the underlying blood vessels.

5 - Stem clamps are applied proximally and distally from the removal area. The mesentery was cut in a V-shape. Small vessels crossing the transection line are clamped and tied.nbsp;

6 - The dissected intestine is held by an assistant, and the surgeon creates small holes in the avascular segments of the mesentery along the line of transection. Small vessels are clamped and tied with a Dexon suture. Note that the incision line in the intestine is oblique, not perpendicular to its axis. The blood supply to the small intestine is such that the antimesetal border of the intestine can become ischemic if the vascular arcade supplying the edge of the resected intestine is perpendicular. The second reason for bowel transplantation at an angle rather than a perpendicular line is that the oblique transection will give a greater width of the anastomosis and reduce the incidence of strictures.

7 - The bowel is transected and the affected part is plugged with a TA-55 surgical stapler and separated from the healthy ileum and caecum.

8 - The affected part of the intestine is removed to the side, and the healthy segment of the proximal ileum (P) is brought to the anastomosis of the healthy segment of the distal ileum (D). The first step in this anastomosis is the placement of a 3-0 Dexon Lembert suture across the mesenteric border approximately 1 cm from the mucosal margin. The purpose of this stitch is to release tension from the future suture line and keep the intestine in a suitable approximation for the rest of the anastomosis.

9 - The bowel is now available for a single-layer end-to-end anastomosis according to Gambee.-
Gumby anastomosis

10 - The first step in the Gambee technique is the suture previously noted in Figure 8 at the mesenteric border of the intestine. This is called here the south (S) seam.
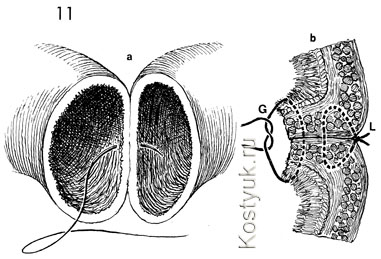
11 - The Gambee technique is a single-layer end-to-end anastomosis; all knots of which are tied inside the intestinal lumen. b - cross section a. Note that the initial Lembert suture (L), located at the mesenteric junction of the intestine, has been tied and therefore tends to invert the mucosal margins. A Gambee (G) suture was placed through the mucosa; the entire intestinal wall exits the serosa, enters the intestinal serosa on the opposite side, passes the intestinal wall, and exits the mucosa. When tied, it further inverts the edge of the bowel.

12 - Each successive Gambee suture is placed approximately 3 mm around the bowel.

13 - Section of the Gumby seam shows the path of the seam. In "a" the suture enters the intestine through the mucosa, passes through the entire intestinal wall, exits the serosa, passes through the serosa of the opposite segment of the intestine, penetrates the entire intestinal wall and exits the mucosa, and "b" Gambee suture is connected to the knot on side of the intestinal lumen, trying to invert the anastomosis.

14 - The process is almost complete around the entire circumference of the intestine.

15 - When all but the 5 mm hole in the bowel wall is sutured, an adjacent marginal suture may be used. The letter "a" in the figure shows the closest edge seam. When tied, it dramatically inverts the entire seam line. The letter "b" is a cross-section of the near extreme inverted seam, which sets out the details of the technique. Note that the proximal dressing suture is the only stitch in the Gambee technique that is tied to the serosal intestinal tissue and not to the mucosa. The suture begins by placing through the serosa from one segment of the intestine about 1 cm from the edge. It penetrates the entire surface and exits the mucous membrane approximately 1 cm from the edge. The suture immediately reverses and passes through the mucous membrane of the same intestinal segment at a distance of 3 mm from the edge, penetrates the entire wall of the same segment and exits the serosa. This is the nearest and farthest coil of this line. The suture is then placed across the proximal edge of the opposite intestinal segment 3 mm from the edge through its serosa to penetrate the entire intestinal wall and exit the mucosa. The needle is immediately placed back through the mucosa about 1 cm from its edge, penetrates the entire intestinal wall and exits the serosa about 1 cm from its edge. Tying the suture dramatically inverts the entire anastomosis.

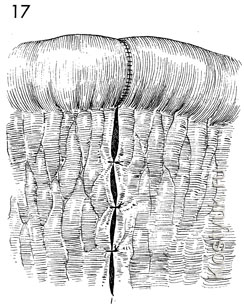
16 - Four Lembert 3-0 Dexon relief sutures are located north (N), east (E), and west (W) of the gut axis. These sutures further invert the anastomosis and relieve tension from the suture line to improve healing.
17 - The mesentery of the small intestine is closed with interrupted 3-0 synthetic rassava sutures to prevent internal hernia.
Sourced from atlasofpelvicsurgery.com
Resection of the small intestine is a surgical intervention in gastroenterology, which is widely used in the detection of tumors. Required to remove part of the intestine affected by the pathological process. According to statistics, there is a high risk of postoperative complications, so the procedure is not carried out without a good reason. Despite the fact that the intestine is long, the removal of the fragment has a negative impact on the general condition of the body.
Indications for carrying out
Resection of the small intestine is performed on an emergency and planned basis. It is required in all cases when it is impossible to carry out conservative treatment of the patient.
Indications for emergency surgery:
- Crohn's disease. This autoimmune process leads to an inflammatory response. The disease may not manifest itself for a long period. With an exacerbation, a clinic of an acute abdomen appears, which requires emergency hospitalization in the department of surgery.
- Inflammatory process of Meckel's diverticulum. This is the residual part of the umbilical-mesenteric duct, which is located at some distance from the caecum.
- Intestinal volvulus. Occurs in the elderly and young children; predisposing factors are anatomical features - elongation of the loops of the small intestine and mesentery. As a result, twisting occurs due to excessive mobility and necrosis of the loops.
- Massive trauma to the intestine or mesentery. If it is not possible to sew up the wound in the usual medical way, the affected area is removed.
- Umbilical hernia, complicated by infringement of the loops of the small intestine. As a result of infringement, the blood supply stops, which within a few hours leads to necrosis of the intestinal loops. During the operation, the afferent section is resected at a distance of 40 cm, and the outlet - at a distance of 15 cm from the site of infringement. To restore intestinal patency, the surgeon imposes a side-to-side anastomosis.
- Thrombosis of the mesenteric vessels. The operation is due to the fact that part of the intestinal loops that feed on clogged mesenteric vessels undergoes necrotic changes. In this case, it is difficult to determine the removal boundary. Doctors perform surgery on older people with comorbidities. In some cases, thrombolysis is performed with attempts to restore blood circulation in necrotic tissues. Success depends on the massiveness of the lesion and the stage of the process.
In a planned manner, a medical operation is prescribed when diagnosing neoplasms. Benign tumors are excised using economical or sectoral resection. Malignant neoplasms are removed using an extended resection of the intestine and mesentery. In this case, it is also required to clamp the arteries and lymphatic ducts in the lesion.
Contraindications
Contraindications to surgical actions include severe concomitant diseases in a state of decompensation, terminal states, including coma. As well as the last stages of oncology, since in this case the tumor is inoperable.
Preparatory stage
To achieve positive dynamics after surgery and reduce the risk of postoperative complications, the patient needs to carefully prepare. If an emergency intervention is carried out, the preparation takes a minimum amount of time and consists in passing tests to calculate the amount of anesthesia.
During planned hospitalization, the patient undergoes a whole list of procedures. Consultations are scheduled with a general practitioner, surgeon, cardiologist, anesthesiologist, blood and urine tests are taken, and an ECG is recorded.
The patient is given a cleansing enema the day before the operation. This is required to prevent postoperative infectious complications.
The patient is obliged to follow a dietary diet and exclude from the diet:
- legumes;
- alcoholic drinks;
- fresh fruits and vegetables.
The last meal and fluid intake is 12 hours before surgery.
In order to prepare the intestines, the patient is assigned to receive special solutions that are drunk in a volume of several liters before the operation.
Also, to exclude infection after the main stage of treatment, antibiotic therapy is prescribed. Some drugs can cause massive bleeding, so the patient should warn the attending physician about the drugs he is taking.
Stages
 Stages of resection of the small intestine:
Stages of resection of the small intestine:
- Use of general anesthesia.
- Access - incision of the abdominal wall in the lower third.
- Revision of the abdominal cavity.
- The principle of mobilization of the mesentery.
- Excision of necrotic areas of the small intestine.
- Formation of anastomosis between functionally or anatomically different areas.
There is an area in the mesentery where the vessels do not pass. A hole is made in it with a clamp. Serous sutures are applied along its edges. Next, the mesentery, marginal vessel and muscle layer are pierced. The surgeon performs manipulations without penetrating into the lumen of the intestinal loop.
Next, a suture is tied on the vessel with penetration into the intestinal wall. These sutures are placed in the distal and proximal bowel. Once the ligatures have stopped circulation within healthy tissue, the mesentery and the necrotic area are transected. Anastomoses are superimposed, the so-called connections of hollow organs. There are three types of them:
- Side to end - used when connecting anatomically different areas.
- End to end - is used most often, as it is physiological, connects the parts as they were before the operation. Among the shortcomings is the possibility of scar formation.
- Side to side - take the leading and leading ends and connect their side surfaces.
A colostomy is the proximal part of the small intestine, which is removed and fixed on the anterior abdominal wall. It can be both permanent and temporary. Through it passes the intestinal contents. The part remote from the affected area is sutured tightly. It is required when it is impossible to restore the functioning of the intestine with the help of anastomoses. If a colostomy is imposed as a temporary measure, after a certain period of time, an operation is performed aimed at restoring the functioning of the intestine using an anastomosis.
Laparoscopic technique is widely used in surgical practice. A small incision is made in the abdomen, into which cameras, instruments, and light are inserted.
Complications after surgery
The consequences depend on the root cause that led to the operation. There may be:
- infectious complications;
- bleeding;
- scarring, which will lead to obstruction of the intestinal contents;
- hernial protrusion at the site of excision.
To reduce the risk, the patient is prescribed daily dressings of the postoperative wound, early activation, and special attention is paid to sparing nutrition. After a few days, the patient consumes only liquid food eight times a day. A month later, the patient can eat broths cooked on meat, jelly. After two years, there is a gradual return to the usual diet.
Resection of the small intestine requires following the recommendations of the attending physician for a successful rehabilitation period.
All surgical interventions that are performed on the intestines can be divided into several categories. So allocate:
Depending on the area of intervention:
- Operations on the large intestine.
- Operations on the small intestine (resection):
- duodenum;
- jejunum;
- ileum.
Depending on the method of implementation:
- Laparotomy (implies classical access by dissection of the abdominal wall).
- Laparoscopy (using a laparoscope through small incisions in the abdominal wall).
- Methods depending on the type of anastomosis:
- "side to side";
- "end to end";
- "side to end";
A laparoscope is a special tool in the form of a tube, to which a light bulb and a video camera are attached, which displays an image on a large monitor. This video guides the surgeon during the operation. During the intervention, special laparoscopic instruments are also used.
The choice of surgical intervention is made by the surgeon based on the results of a complete examination, taking into account all tests, the presence and nature of concomitant pathologies, the age, weight of the patient and other necessary data.
Preparation for resection
Such an operation is a serious intervention in the patient's body. Therefore, before making it, doctors thoroughly examine the patient. The following analyzes and studies are mandatory:
- general blood analysis;
- blood clotting test;
- liver tests;
- general urine analysis;
- gastroscopy or colonoscopy (depending on the pathology of the small or large intestine);
- electrocardiogram;
- X-ray examination of the abdominal and chest cavity;
- CT, MRI, if necessary, at the discretion of the doctor.
If, during the collection of anamnesis or during the examination, concomitant diseases are detected in a patient, consultation of specialized specialists is indispensable!
In addition to the examination, the period of preparation for the operation includes:
- Power correction. A week before the scheduled date of the operation, you should refuse products that contain fiber. 12 hours before the intervention - do not eat or drink anything.
- Refusal to take medications that affect blood clotting.
- Enema and/or laxatives.
- Taking antibiotics is not mandatory, but it is often prescribed by a doctor.
A full examination, compliance with all the doctor's recommendations during the preparation period, will help prevent possible complications. With urgent (urgent) operations, preparation is minimal, because any delay can affect the outcome of the intervention. The most common indications for emergency operations are peritonitis, necrosis (as a result of intestinal infarction), etc.
A preliminary consultation with an anesthesiologist is also required, as a result of which the doctor will make a conclusion about the possibility, type, dose of an anesthetic for general anesthesia.
Resections of the small intestine
Resection is resorted to only if conservative therapy has not been effective. Urgent operations are also performed when the disease threatens the life of the patient, for example, internal bleeding with an open duodenal ulcer, acute obstruction, necrosis.
Laparoscopy is less traumatic for the patient and the rehabilitation period is noticeably shorter compared to abdominal surgery
Indications for resection of the small intestine may include:
- Mesenteric infarction (as a result of intestinal necrosis).
- Acute trauma.
- Polyp with signs of malignancy.
- Peptic ulcer with perforation.
- Acute obstruction.
- Crohn's disease.
Resection of the small intestine is performed under general anesthesia, so during the procedure the patient does not feel pain, but is in a state of sleep. The duration of the operation can vary from 1 to 4 hours, depending on the extent of the surgical intervention. 
The chosen method also significantly affects the duration. With laparotomy, the time is noticeably reduced due to greater convenience for the surgeon, a better view.
Almost every forum on the Internet that discusses health issues after bowel resection is replete with enthusiastic reviews from those who underwent surgery by laparoscopy. But when removing a malignant tumor, this threatens with the possibility of incomplete removal of the lymph nodes, leaving the adjacent neoplasm unnoticed, which subsequently worsens the prognosis of the patient's implantation. Therefore, do not be seduced by beautiful videos in which laparoscopy looks safe and not so bloody. The choice should be your surgeon - trust the professional!
Resection of the large intestine
The most common indication for resection of the large intestine is malignant neoplasms, so laparoscopic surgery is rare. This is due to the need to remove not only the tissue damaged by the tumor, but also the lymph nodes “scattered” along the mesentery in order to prevent relapses, and it is very problematic to perform such manipulations through the laparoscope.
Indications for resection may be:
- Malignant neoplasms.
- Inflammatory bowel disease.
- Acute intestinal obstruction.
- Necrosis.
- Diverticulitis.
- Benign neoplasms.
- Congenital malformations.
- Intestinal intussusception.
The operation is performed under general anesthesia and usually takes several hours. A feature of the technique of its implementation is the mandatory washing of the entire abdominal cavity with an antiseptic in order to prevent the development of possible complications. This stage is necessary, since the large intestine is densely populated with a wide variety of microflora, including conditionally pathogenic ones. In addition, during resection of the large intestine, drainage tubes are necessarily installed in the abdominal cavity, through which the exudate will be removed.
Separately, it is necessary to single out operations on the rectum, since the anal sphincter is located here, this department is tightly fused with the tissues of the pelvic floor, and these factors complicate the task. The most unfavorable prognosis is given if the pathological process captures the lower third of the organ, and it is not possible to save the sphincter. In this case, surgeons try to perform plastic surgery in order to minimize inconvenience for the patient during defecation. In the case when the anal sphincter is preserved, the rehabilitation process is easier, and the patient's standard of living after it is much higher.
Progress of the intervention
Regardless of the type of operation and the method of its implementation, the first step is to connect all the necessary infusions, and introduce the patient into anesthesia. After that, an antiseptic treatment of the surgical field is carried out and either one large (with laparotomy) or several (usually 2-3, but not more than 6 - with laparoscopy) incisions are made.
 After that, the area of the organ to be removed is found, a clamp is applied above and below the excision borders to prevent bleeding. It must be borne in mind that apparently healthy tissue may actually be non-viable (necrosis can lead to this), so excision is performed “with a margin”. Also, a part of the mesentery is to be removed along with the vessels feeding the intestine, which must first be tied up. Excision should be made as carefully as possible in order to prevent tissue necrosis. If possible, after removing part of the intestine, the two free ends are immediately connected by choosing the appropriate type of anastomosis (for interventions on the small intestine, only the side-to-side and end-to-end types are used).
After that, the area of the organ to be removed is found, a clamp is applied above and below the excision borders to prevent bleeding. It must be borne in mind that apparently healthy tissue may actually be non-viable (necrosis can lead to this), so excision is performed “with a margin”. Also, a part of the mesentery is to be removed along with the vessels feeding the intestine, which must first be tied up. Excision should be made as carefully as possible in order to prevent tissue necrosis. If possible, after removing part of the intestine, the two free ends are immediately connected by choosing the appropriate type of anastomosis (for interventions on the small intestine, only the side-to-side and end-to-end types are used).
If at this stage it is impossible to perform such a manipulation, or there is a need to delay it, allowing the intestine to recover, then a temporary or permanent ileostomy is applied (with interventions on the rectum - a colostomy). In the case of a temporary one, in the future, repeated surgical intervention is necessary to restore the integrity of the organ with one of the types of anastomosis.
At the end of the operation, the patient, if necessary, installs drainage tubes into the abdominal cavity, in case of resections of the small intestine - into the stomach cavity - to pump out the fluid. After that, sutures are applied. The outcome of the operation depends on the coherence of the work, the attentiveness of the medical staff, the correctness of the chosen technique.
It is extremely important during the intervention to wash the abdominal cavity as often as possible, carefully isolate the operated area with tampons to prevent peritonitis and other infectious complications!
Possible Complications
Thorough examination, preparation for surgery, trained medical staff, high professionalism of the doctor, unfortunately, do not guarantee the absence of complications. Having studied the data of medical statistics, we can say that certain difficulties lie in wait for 90% of those operated on for this reason.
The most common complications are:
- Attachment of infection (most often suppuration of sutures, peritonitis). High fever, increased pain. Redness, swelling are the first signs of the development of this condition.
- Hernia development. Even correctly applied sutures and excellent tissue fusion do not guarantee the same strength of the abdominal wall as it was before the operation. Therefore, the incision site is often transformed into a hernial orifice.
- Adhesions and scars. They can not only cause pain, pulling sensations, but also disrupt intestinal patency and cause other unpleasant consequences; in this condition, the temperature may rise.
- Bleeding. It is also a common occurrence after bowel resection, which can even cause death in case of untimely assistance.
After the operation, at least a week, and most often 10 days, which the patient spends in a hospital. This allows doctors to keep the patient's condition under constant control and, if necessary, adjust the treatment.
Recovery period
 At this time, the patient should be as attentive to his body as possible. High temperature, constant increasing pain, poor general well-being should alert. Each of these signs may indicate that complications are developing and worsen the prognosis for recovery.
At this time, the patient should be as attentive to his body as possible. High temperature, constant increasing pain, poor general well-being should alert. Each of these signs may indicate that complications are developing and worsen the prognosis for recovery.
Also, we must not forget that during the rehabilitation the patient is shown bed rest, and this can also cause undesirable consequences. Most often it will be constipation and pneumonia. If in the first case vaseline oil can be effective, then in the second case - inflating balloons, breathing exercises. Pneumonia and constipation are the result of stagnation in the pulmonary circulation and insufficiency of peristalsis due to a long forced horizontal position.
The first signs indicating the diagnosis of "pneumonia" may be shortness of breath, subfebrile or high temperature, wheezing during inspiration. That is why morning rounds in the hospital and attention to the patient of relatives and relatives at home after discharge are absolutely necessary.
If, after being discharged from the hospital, you find a fever, a violation of the integrity of the seams, a sharp deterioration in well-being, do not endanger your health - call an ambulance immediately!
Nutrition in the postoperative period
Although it is desirable to reduce the load on the patient's intestines after surgery, providing the body with all the nutrients is essential. With extensive resections in the first week, the patient is fed parenterally, when this period has passed, a normal diet is gradually established. And only six months after the operation, you can return to the usual menu, provided that there are no complications from the digestive system.
 It is best to plan your meals so that the daily amount of food is divided into 6-8 servings. Before a meal, any dish must be thoroughly chopped (using a blender, rubbing through a sieve). Gradually, from pureed dishes, they move on to finely chopped ones, it can be soup vegetables, as well as cereals, to which butter can be added.
It is best to plan your meals so that the daily amount of food is divided into 6-8 servings. Before a meal, any dish must be thoroughly chopped (using a blender, rubbing through a sieve). Gradually, from pureed dishes, they move on to finely chopped ones, it can be soup vegetables, as well as cereals, to which butter can be added.
It is forbidden to use during the recovery period:
- everything that contains large amounts of fiber - cabbage, cucumbers, radishes, all fruits and vegetables with skins;
- soda, as well as a fermentation product - to prevent the occurrence of flatulence;
- everything that enhances peristalsis - carrot and beet juice, prunes;
- fatty, fried, smoked foods are also contraindicated.
In a word, you need to eat only healthy foods that are not difficult to digest.
Dishes allowed in the postoperative period: salads from boiled vegetables, which can be seasoned with vegetable oil; lean meats and fish in the form of steam cutlets, meatballs; mashed potatoes, zucchini, pumpkins; you can also eat vegetable soup, puree soup; lactic acid products will also help not only replenish the supply of nutrients, but also restore the microflora of internal organs.
You should not go to any forum for advice on proper nutrition after surgery, your gastroenterologist will help you make a diet, since only he can take into account all the characteristics of your body.
Resection is a serious, but very often necessary measure to save a person's life. Regular medical examinations, attention to your body will help you notice the development of the disease in the early stages, which will prevent the need for surgical intervention. But if the need for it nevertheless arose, do not delay the inevitable, because time often does not play in favor of patients. Be healthy!
Resection or excision of a section of the small intestine is performed in case of wounds, necrosis in cases of infringement and thrombosis of blood vessels, and tumors.
Operation technique. The section of the intestine to be removed is taken out into the wound and covered with gauze napkins. The boundaries of resection should be within the intestine, not involved in the pathological process. The removed section of the intestine is cut off from the mesentery. When a small area is resected, it is separated from the mesentery near the edge of the intestine. With the removal of a significant portion of the intestine, the part of the mesentery belonging to it should also be removed, excising it at an angle to the root of the mesentery. The dissection of the mesentery is performed between clamps applied to its vessels or tied with threads brought under the vessels with a Deschamps needle. The area of the intestine to be removed is clamped with intestinal clamps. The further technique of the surgeon depends on the choice of the created anastomosis.
Anastomosis or fistula end to end(end-to-end). Soft intestinal clamps are applied obliquely to the length of the organ, outside the affected area of the intestine. At the same time, 2 clamps are installed on each side of the resected segment of the intestine at intervals of 1.5-2 cm. A segment of the intestine is cut off along the central clamps. The oblique position of the terminals makes the diameter of the intestine at the site of the section wider, which further prevents the narrowing of the digestive tube resulting from the layering of the anastomosis sutures. Peripheral clamps with the ends of the intestine lead to each other, preventing twisting of the intestine. Holders - interrupted sutures, picking up the wall of both ends of the intestine through the mesenteric and free edges of the intestine, strengthen the position of the anastomosis. A serous-muscular suture is applied from the holder to the holder, capturing the walls of the ends of the intestine 3 mm below the edges of the inner lips of the anastomosis. Then a continuous suture is applied through the entire thickness of the wall of the inner lips of the anastomosis, which then passes into the screwing Schmiden suture for the outer lips of the anastomosis. They remove the clamps from the intestine, check the patency of the anastomosis, change sterile wipes, the surgeon washes his hands. The continuation of the serous-muscular suture, which closes the screwed suture, completes the creation of the anastomosis. A defect in the mesentery is sutured with rare interrupted sutures. The wound of the abdominal wall is sutured in layers.
Rice. 152. Resection of the small intestine. Mesenteric ligation technique.
I - clamping of the mesentery and its intersection; II - the imposition of a ligature on the area with crossed vessels; III - stages of excision of a section of the intestine. Immersion of the stump of the intestine in a purse-string suture.
Anastomosis side to side(fig. 153) (side-to-side). Outside the affected area, the intestine is clamped with crushing clamps at a right angle to its length. In place of the removed clamps, ligatures are applied, which, when tied, block the intestinal lumen. Departing 1.5 cm to the periphery from these ligatures, a serous-muscular purse-string suture is applied. Inwards from the tied thread, a soft clamp is applied and the intestine is crossed along it. The resulting stump of the intestine is smeared with iodine tincture and immersed with a purse-string suture, which is tightened over it. Over impose nodal serous-muscular sutures. The other end of the intestine is treated in the same way. Curved soft clamps are applied to the central and peripheral blind ends of the intestine along their free edge and brought to each other isoperistaltically, i.e., along the peristalsis. The stumps of the intestine are brought together with holders at an interval of 8-9 cm. A serous-muscular suture is applied from one holder to the other. At both ends of the intestine, incisions are made to open the lumen of the intestine, following 0.5-0.75 cm indented and parallel to the serous-muscular suture. These incisions should end without reaching the beginning and end of the performed suture by 1 cm. The inner lips of the anastomosis are sutured with an Albert suture, and its outer lips with a Schmiden suture. After changing the napkins and washing the hands, the clamps are removed and the final serous-muscular suture is performed. Several stitches sew up the hole in the mesentery. The wound of the abdominal wall is sutured in layers. Side-to-side anastomosis is somewhat easier to perform than end-to-end, and less likely to lead to narrowing of the intestinal lumen.

Rice. 153. Resection of the small intestine with side-to-side anastomosis.
a - the first clean interrupted sutures according to Lambert; b - opening of the lumens of both connected intestinal loops; 1 - front (outer) lips; 2 - rear (inner) lips; c - stitching the posterior lips with a continuous twisting seam; g - stitching the anterior lips with a continuous screwing, Schmiden's suture; e - the imposition of a second clean nodal suture according to Lambert.
Relevance of the topic:
Lesson duration: 2 academic hours.
General goal:
Logistics of the lesson
2. Tables and dummies on the topic of the lesson
3. A set of general surgical instruments
Technological map of the practical lesson.
| No. p / p. | Stages | Time (min.) | Tutorials | Location |
| 1. | Checking workbooks and the level of students' preparation for the topic of the practical lesson | Workbook | study room | |
| 2. | Correction of knowledge and skills of students by solving a clinical situation | Clinical situation | study room | |
| 3. | Analysis and study of material on dummies, a corpse, viewing demonstration videos | Models, cadaveric material | study room | |
| 4. | Test control, solution of situational problems | Tests, situational tasks | study room | |
| 5. | Summing up the lesson | - | study room |
Clinical situation
A patient with a closed abdominal injury was admitted to the surgical department. According to emergency indications, a median laparotomy was performed. During the revision of the abdominal organs, bleeding from the vessels of the mesentery, separation of the mesentery from the wall of the small intestine was detected.
Tasks:
1. What is the surgical tactics of the surgeon?
2. What methods of resection of the small intestine are known?
The solution of the problem:
1. Stop bleeding from the vessels of the mesentery, perform a marginal resection of the small intestine, restore the integrity of the intestine by end-to-end anastomosis.
2. Marginal and wedge-shaped.
Intestinal suture and types of anastomoses
Most operations on the organs of the gastrointestinal tract by their nature are one of the following types: opening (tomy) followed by suturing of the cavity, for example, gastrotomy - opening the stomach: fistula (stomy) - connection of the organ cavity through an incision in the abdominal wall directly with the external environment , for example, gastrostomy - fistula of the stomach, colostomy - fistula of the colon, cholecystostomy - fistula of the gallbladder: the imposition of fistula (anastomosis) between the sections of the gastrointestinal tract, for example, gastroenteroanastomosis (gastroenterostomy) - gastrointestinal fistula, enteroenteroanastomosis - interintestinal fistula, cholecystoduodenostomy - fistula between the gallbladder and the duodenum; excision of a part or a whole organ (resection, ectomy), for example, resection of the intestine - excision of a section of the intestine, gastrectomy - removal of the entire stomach.
Intestinal suture It is used on all organs, the walls of which consist of three layers: peritoneal, muscular and muco-submucosal. The intestinal suture is used to close wounds of these hollow organs, both of traumatic origin, and mainly made during surgery, for example, when applying anastomoses (fistulas) between different parts of the intestine, between the intestine and stomach.
The main types of intestinal sutures are shown in fig. 3-14.
Rice. 3. Seam Jobert (Jobert, 1824)

Rice. 4. Seam Pirogov (1849)

Rice. 5. Schmiden's suture
a - general view, b - the course of the thread, c - contact of the cell membranes after tightening the thread.

Rice. 6. Through marginal intestinal suture Gumby
(From: Kirpatovsky I.D. Intestinal suture and its theoretical foundations. - M., 1964.)


Rice. 7. Connell suture
(From: Littmann I. Abdominal surgery. - Budapest, 1970.)


Rice. 8. Reverden-Multanovsky seam
(From: Schmitt V.V., Hartig V., Kuzin M.I. General surgery. - M., 1985.)

Rice. 9. Continuous furrier intestinal suture
(From: Littmann I. Abdominal surgery. - Budapest, 1970.)

Rice. 10. Seam Lambert (Lembert, 1825)

Rice. 11. Purse suture (Doyen)

Rice. 12. Z-stitch

Rice. 13. Double stitch Albert
(From: Kirpatovsky I.D. Intestinal suture and its theoretical foundations. - M., 1964.)


Rice. 14. Double row seam Czerny
a - general scheme, b - second row of sutures. (From: Kirpatovsky I.D. Intestinal suture and its theoretical foundations. - M., 1964; Simich P. Intestinal surgery. - Bucharest, 1979.)
When applying the intestinal suture, it is necessary to take into account the sheath structure of the walls of the digestive tract, consisting of the outer serous-muscular layer and the inner - muco-submucosal. It is also necessary to keep in mind the various biological and mechanical properties of their constituent tissues: the plastic properties of the serous (peritoneal) cover, the mechanical strength of the submucosal layer, the tenderness and instability of the epithelial layer to injury. With an intestinal suture, layers of the same name should be connected.
Currently, the generally accepted is a two-row, or two-tier, Albert seam , representing a combination of two types of intestinal sutures: through all layers - the serous, muscular and mucous membranes - the suture of Jelly and the serous-serous suture of Lambert .
With a serous suture of Lambert on each of the sutured walls, the injection and puncture is done through the peritoneal integument of the walls; so that the suture does not cut through, the muscular layer of the intestinal wall is also captured, therefore this suture is usually called serous-muscular.
The seam of Jelly (or Cherni) is called internal. It is infected, "dirty", Lambert's suture is external, uninfected - "clean".
The internal (through) seam, passing through the submucosal layer, provides mechanical strength. It does not allow the edges of the intestinal incision to disperse under the influence of peristalsis, intra-intestinal pressure. This seam is also hemostatic, because. captures and compresses large blood vessels in the submucosal layer.
The external serous-muscular suture creates hermeticism: when it is applied, the main condition is wide contact of the peritoneum adjacent to the wound; due to its reactivity and plastic properties, in the first hours after the operation, gluing occurs, and later on, a strong fusion of the walls being stitched. Under the protection of the outer suture, the process of fusion of the inner layers of the intestinal wall takes place.
The internal suture, which comes into contact with the infected contents of the intestine, must be made of absorbable material (catgut), so that it does not become a source of a long-term inflammatory process in the future. When stitching the edges of the serous-muscular layer, a non-absorbable material is used - silk.
When applying an intestinal suture, it is necessary to ensure thorough hemostasis, minimal trauma and, mainly, asepsis.
The conventional two-row seam satisfies these requirements in most cases. However, in some cases complications arise: insufficiency of the suture, development of narrowing in the anastomosis (stenosis), adhesions in the circumference of the anastomosis. The processes accompanying the healing of the intestinal wound, the fate of the sutures, have been little studied until recently. Modern studies have revealed serious shortcomings of the through intestinal suture: such a suture causes severe trauma to the mucosa, its necrosis, rejection with the formation of defects - ulcers that penetrate deep into the intestinal wall. The tortuous channel of the suture serves as a way for the infection to penetrate into the depth of the intestinal wall; as a result of this, in the tissue shaft protruding into the lumen of the anastomosis, an inflammatory process develops from all three layers of the intestinal wall and wound healing occurs by secondary intention. Epithelialization and formation of glands are delayed up to 15-30 days instead of 6-7 days according to the norm, and the stitched areas turn into a rough unyielding scar. For normal healing of the intestinal wound, it is necessary to abandon the traumatic through twisting suture: the layers of the intestinal sheath must be connected separately, independently of each other. An isolated submucosal suture - a submucosal suture or submucosal suture with the mucosa provides, under the condition of a gentle technique, i.e. without the use of clamps, with taking only the very edge of the mucosa into the seam, the absence of necrosis, primary tension, the formation of a gentle linear scar within 6-9 days and the rapid disappearance of the tissue shaft protruding into the lumen of the anastomoses.
Rice. 15. Types of intestinal anastomosis
a - end to end, b - side to side, c - end to side. (From: Littmann I. Abdominal surgery. - Budapest, 1970.)
The imposition of terminal and lateral anastomosis is used for resection of the small intestines, when the stomach is connected to the intestine, and bypass anastomoses are applied on the large intestines.
The third type of anastomosis - end to side, or “termino-lateral”, is used for resection of the stomach, when its stump is sewn into the side wall of the small intestine, when connecting the small intestine to the large intestine, when connecting the large intestines after resection (Fig. 18).

Rice. 16. Anastomosis end to end
a - connection of sections of the intestine with serous-muscular sutures of Lambert, b - suturing of the posterior wall of the anastomosis with a Reverden-Multanovsky suture, c - suturing of the anterior wall of the anastomosis with a screwing Schmiden suture. d- Lambert serous-muscular sutures on the anterior wall of the anastomosis.

Rice. 17. Anastomosis side to side
a - connecting sections of the intestine with Lambert's serous-muscular sutures, b - suturing the posterior wall of the anastomosis with a Reverden-Multanovsky suture, c - suturing the anterior wall of the anastomosis with a screwing Schmiden suture, d - applying the second row of Lambert's serous-muscular sutures to the anterior wall of the anastomosis. (From: Kotovich L.E., Leonov SV., Rutsky A.V. et al. Technique for performing surgical operations. - Minsk, 1985.)



Rice. 18. Stages of end-to-side anastomosis
Resection of the small intestine
Indications. Tumors of the small intestine or mesentery, necrosis of the intestine with obstruction, strangulated hernia, thrombosis of the supply vessels (arteries), multiple gunshot wounds.
Anesthesia. Narcosis, local anesthesia.
Operation technique. The incision is made along the midline of the abdomen, retreating 2-3 cm from the pubis, with a continuation above the navel. After opening the abdominal cavity, the section of the small intestine to be resected is taken out into the wound and carefully isolated with gauze napkins. Outline the boundaries of resection within healthy tissues. The resected section of the intestine is separated from its mesentery, having previously tied up all the blood vessels located near the edge of the intestine. Vessel ligation is performed using a Deschamp needle or curved clamps. The mesentery is crossed between the clamps and ligatures are applied (Fig. 19-20).
You can do otherwise: make a wedge-shaped dissection of the mesentery in the area of the removed loop, tying all the vessels located along the incision line. Carefully isolate the field of operation with gauze compresses. The contents of the intestine are squeezed into adjacent loops. A crushing clamp is applied to both ends of the removed part, and an elastic pulp is applied to the ends of the remaining part of the intestine to prevent the contents from flowing out. Then, at one end, the intestine is cut off along the crushing pulp and a stump is formed from the remaining part. To do this, its lumen is sutured with a through continuous catgut suture, making each stitch a puncture of the wall from the inside (furrier's suture, or Schmiden's suture); with this suture, the intestinal wall is screwed inward. The seam starts from the corner, a knot is made there, and ends at the opposite corner also with a knot, tying the loop to the free end of the thread.
The stump can also be sutured with a continuous continuous suture. The goal of these methods of suturing the stump is to make it as small as possible and leave as little dead space as possible for the subsequent lateral enteroenteroanastomosis. The sutured end of the stump is closed over top with interrupted serous-muscular sutures. . Even faster, you can process the stump by bandaging the intestine along the place crushed by the pulp with a strong catgut thread and immersing the stump resulting after cutting off into a pouch. This method is easier to perform, but the stump is more massive and the blind end is larger.


Rice. 19. Stages of resection of the small intestine
a - the formation of a hole in the mesentery of the small intestine, b - the imposition of an enteromesenteric suture. (From: Littmann I. Abdominal surgery. - Budapest, 1970.)

Rice. 20. Stages of resection of the small intestine
a - correct intersection of the intestine (slope of the line of intersection from the mesenteric edge to the opposite), b - incorrect (slope of the line of intersection from the antimesenteric edge to the mesenteric). (From: Simic P. Bowel Surgery. - Bucharest, 1979.)
After removal of the resected intestine, a second stump is formed, the covering napkins are replaced and the lateral anastomosis is applied. The central and peripheral segments of the intestine are freed from the contents, elastic intestinal sphincter is applied to them and applied to each other by the side walls isoperistaltically, i.e. one on the continuation of the other, while avoiding their twisting along the axis. The walls of the intestinal loops for 8 cm are connected to each other by a number of interrupted silk serous-muscular sutures according to Lambert (the first "clean" suture) ; sutures are placed at a distance of 0.5 cm from each other, retreating medially from the free (antimesenteric) edge of the intestine. Secondary napkins are placed on the stitched intestines, and on an instrument table covered with a towel, all instruments are prepared for the second, infected (contaminated), stage of the operation. In the middle of the line of applied serous-muscular sutures, at a distance of 0.75 cm from the suture line, two anatomical forceps are used to grab the fold of the wall of one of the intestinal loops transversely to the axis of the intestine and cut it with straight scissors through all layers parallel to the line of serous-muscular sutures. Having opened the lumen of the intestine for some length, a small tupfer is introduced into it and the cavity of the intestinal loop is drained; after that, the incision is lengthened in both directions, not reaching 1 cm to the end of the line of serous-muscular sutures. In the same way, the lumen of the second intestinal loop is opened. . They begin to sew the inner edges (lips) of the resulting holes with a continuous twisting catgut seam through all layers (Jelly seam). The seam is started by connecting the corners of both holes ; pulling the corners together, tie a knot, leaving the beginning of the thread uncut. When performing a twisting seam, make sure that all layers are pierced on each side. To avoid corrugation of the seam line and narrowing of the anastomosis, the thread should not be overtightened. Having reached the opposite end of the holes to be connected, fasten the seam with a knot and proceed with the same thread to connect the outer edges (lips) of the holes with a Schmiden furrier screw-in stitch (the second “dirty” stitch) . To do this, a puncture is made from the side of the mucous membrane of one intestine, then from the side of the mucous membrane of the other intestine, after which the seam is tightened; the edges of the hole are screwed inward. Having reached the beginning of the "dirty" seam, the end of the catgut thread is tied with a double knot with its beginning. Thus, the lumen of the intestinal loops is closed and the infected stage of the operation ends.
Tools are replaced, contaminated covering napkins are removed; hands are washed with an antiseptic solution, intestinal pulps are removed and proceed to the last stage - the imposition of a number of interrupted serous-muscular sutures (the second "clean" suture) already on the other side of the anastomosis . These sutures close the newly applied Schmiden suture. Punctures are made at a distance of 0.75 cm from the line of the “dirty” seam.
Thus, the edges of the anastomosis are connected throughout by two rows of sutures: internal - through and external - serous-muscular. Blind ends (stumps) in order to avoid their invagination are fixed with several sutures to the intestinal wall. After anastomosis is applied, the hole in the mesentery is closed with several interrupted sutures; check with fingers the width (patency) of the anastomosis. At the end of the operation, the covering napkins are removed, the intestinal loops are introduced into the abdominal cavity, the abdominal wall incision is sutured in layers. One of the negative aspects of the lateral anastomosis is that erosion and bleeding can develop in the mucosa of the blind sacs.
When resection of the small intestine is often used terminal anastomosis. The first moments of the operation before cutting off the part to be removed are performed as described above. Cutting off the central and peripheral ends during resection of the small intestine is carried out along an oblique line: due to this, the gaps are wider and the intestinal suture does not cause narrowing. Intestinal loops are applied to each other with the ends facing the same direction, connected along the edges, retreating 1 cm from the cut line, with silk serous-muscular sutures-holders and a two-row intestinal suture is applied to the anterior and posterior lips of the anastomosis, as described above for lateral enteroenteroanastomosis .
Particular attention should be paid to the connection of the gaps in the region of the mesenteric region, where there is no peritoneum: for peritonization in this area, the area of the adjacent mesentery should also be captured in the suture.
Currently, for suturing, for suturing stumps along the gastrointestinal tract, as well as for the formation of anastomoses, special staplers are used. To close the lumen of the intestine, for example, the small one - during its resection, the duodenum - during the resection of the stomach, the apparatus UKL-60, UKL-40 is used (UKL was originally created for suturing the root of the lung). The device is loaded with tantalum brackets shaped like the letter "P". Tantalum brackets are neutral in relation to tissues and do not cause an inflammatory reaction.
The stapler consists of two main parts: staple and persistent. On the bracket part there is a store for brackets and a pusher connected to the handle. On the hook of the thrust part there is a matrix with grooves, resting against which, the brackets, having passed through the sewn tissues, are bent and take the shape of the letter “B”. Stitched tissues - the walls of the intestine - are placed between the matrix of the thrust part and the staple magazine; by rotating the nut, these parts are brought together, covering the stitched fabrics; the handle is squeezed to the stop, while the brackets are pushed out of the magazine and stitched; without removing the apparatus, a crushing clamp (Kocher) is applied to the removed part and the intestine is cut off along the line of the superimposed apparatus. The apparatus is removed and the resulting cult is immersed with interrupted serous-muscular sutures. The duodenal stump is sutured with the same apparatus.
Apparatus UKZH-7 (suturing the stump of the stomach) imposes a two-row suture with immersion of the first row. Apparatus for the mechanical application of intestinal and gastrointestinal anastomoses have also been created.
Suturing wounds of the small intestine
The abdominal cavity is opened with a median incision and all intestines are examined; damaged ones are temporarily wrapped in a napkin and set aside. After the revision, sequentially treat the detected wounds.
With a small stab wound, it is enough to apply a purse-string serous-muscular suture around it. When tightening the pouch, the edges of the wound are immersed with tweezers into the intestinal lumen.
Cut wounds a few centimeters long are sutured with a two-row suture:
1) internal, through all layers of the intestinal wall - catgut with the introduction of the edges according to Schmiden;
2) external, serous-muscular - nodal silk sutures are applied. You can also use a single-row serous-muscular suture. To avoid narrowing of the intestine, longitudinal wounds should be sutured in the transverse direction.
With multiple closely spaced wounds of one loop, it is resected (Fig. 21).



Rice. 21. Scheme of suturing the wound of the intestine
A - suturing-holders;
B - Schmiden suture on the edges of the wound (first row of sutures);
C - suturing Lambert (beginning of suturing);
D - tying Lambert sutures (second row of sutures).
Theoretical questions for the lesson:
1. Definition of the term “intestinal suture”.
2. Indications for intestinal sutures.
3. Classification of intestinal sutures.
4. General requirements for intestinal sutures.
5. The biological basis of the Lambert suture.
6. Stages of surgical resection of the small intestine.
7. Types of mobilization.
8. Mistakes and complications during the operation of resection of the small intestine.
Practical part of the lesson:
1. Master the technique of ligation of blood vessels in the mesentery.
2. Master the technique of applying various types of intestinal sutures.
3. Master the technique of applying end-to-end, end-to-side and side-to-side anastomoses.
Questions for self-control of knowledge
1. Classification of intestinal sutures.
2. Which seams are related to the seams of the first row?
3. Name the types of aseptic sutures.
4. Which type of anastomosis is the most physiological?
5. How is the inner lip of the anastomosis sutured?
6. Name the order of sutures on the outer lip of the anastomosis.
7. Indications for resection of the small intestine.
8. When is wedge bowel mobilization used?
9. Mistakes and complications during the operation of resection of the small intestine.
Tasks for self-control
Task 1
A patient was admitted to the surgical department with complaints of acute abdominal pain. Objectively: the abdomen is swollen, painful on palpation, muscle tension of the abdominal wall, Shchetkin's symptom is positive. During an emergency laparotomy, thrombosis of the superior mesenteric artery was found. List the sections of the intestine in which blood circulation may be impaired.
Task 2
After surgical treatment and suturing of the wound of the descending colon, a 68-year-old patient developed severe intestinal paresis. On the third day after the operation, there were symptoms of peritoneal irritation, increasing leukocytosis, fever up to 39°C. Specify the possible ways of exudate spreading in case of peritonitis caused by divergence of colon sutures.
Task 3
During surgery for a strangulated oblique inguinal hernia, a loop of the small intestine with signs of necrosis (absence of peristalsis, thrombosis of the mesenteric veins, violation of the integrity of the intestinal wall) was found in the hernial sac. In view of the discrepancy between the diameters of the lumen of the afferent and efferent loops, the surgeon, after resection of the intestinal section, imposed an interintestinal anastomosis of the “side-to-side” type, the fistula size was 2.5 times the width of the lumen of the outlet loop. In the postoperative period, there was intestinal obstruction in the area of the anastomosis. What are the likely causes of this complication, how can they be prevented?
Samples of correct answers
Task 1
Circulatory disorders in the jejunum, ileum, blind, ascending colon, % of the transverse colon and appendix.
Task 2
The inflammatory process develops in the left mesenteric sinus and can pass into the pelvic cavity, into the right mesenteric sinus.
Task 3
As a result of the intersection of the circular muscle layer over a large extent, intestinal paresis occurs in the fistula area with the development of dynamic intestinal obstruction.
Test tasks for self-control
Literature
Main:
1. Kulchitsky K.I., Bobrik I.I. Operative surgery and topographic anatomy. Kyiv, Vishcha school. - 1989. - p. 225-231, p. 254-258.
2. Kovanov V.V. (ed.). Operative surgery and topographic anatomy. - M.: Medicine. - 1978. - p. 342-346, p. 349, p. 356, p. 367-368.
3. Ostroverkhov G.E., Bomash Yu.M., Lubotsky D.N. Operative surgery and topographic anatomy. - Moscow: MIA. – 2005, p. 568-584.
4. Sergienko V.I., Petrosyan E.A., Frauchi I.V. Topographic anatomy and operative surgery. / Ed. Lopukhina Yu.M. - Moscow: Geotar-med. - 2001. - 1, 2 volumes. – 831, p. 99-111, p. 186-193.
Additional:
1. Shalimov A.A., Redkin S.N. Atlas of surgical operations on the abdominal organs. // Health - Kyiv. 1965, p. 15-17, p. 321-328.
2. Velker F.I., Vishnevsky A.S. and etc. (Edited by Shevkunenko V.N.) - "Medgiz" - 1951. - p. 340-344, p. 368-376.
Internet Library
Notes
Notes
TOPIC: “Operations on the abdominal organs. Intestinal sutures. Resection of the small intestine»
Relevance of the topic: The most common complication of surgical interventions on the hollow organs of the digestive system is the failure of the intestinal suture. In this regard, it is important to master the technique of applying an intestinal suture.
Lesson duration: 2 academic hours.
General goal: To study the theoretical basis and master the technique of intestinal sutures, intestinal anastomoses, the stages of small intestine resection surgery.
Specific goals (to know, be able to):
1. Know their anatomical and physiological features of the structure of the walls of hollow organs.
2. Know the basic requirements for intestinal sutures.
3. Be able to apply various types of intestinal sutures and anastomoses.
4. Know the indications for resection of the small intestine.
5. To be able to conduct an audit of the jejunum and ileum, using Gubarev's technique.
6. To know the stages of the operation of resection of the small intestine and the technique of their implementation.
7. Be able to form three types of anastomosis.
