Large pelvis contains. Pelvic floor, bony pelvis
Taz, pelvis, is formed by the pelvic bones, sacrum, coccyx, and ligaments. It is divided into a large pelvis, pelvis major, and a small one, pelvis minor. The border between them is the border line, linea terminalis, which runs from the cape to the arcuate line and further to the pubic tubercle. The pelvic cavity is a container for internal organs, and the muscles of the abdomen and thigh are attached to its bones. The pelvis has two openings: the upper one, apertura pelvis superior, bounded by the boundary line, and the lower one, apertura pelvis inferior, bounded behind by the coccyx, on the sides by the ischial tubercles, in front by the branches of the ischial and pubic bones. In the pelvis in men is: the rectum, bladder, prostate, vesicular gland and vas deferens, and in women - the rectum, uterus, oviduct, bladder, ovaries, vagina.
Also in the pelvis are blood and lymphatic vessels, nodes, nerves and nerve plexuses.
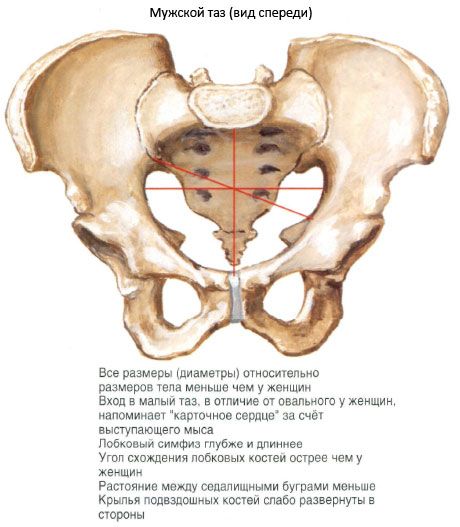
In the structure of the pelvis, pronounced sex differences are noted. In the early childhood the pelvis in both sexes is almost the same. AT puberty sexual characteristics of the structure of the pelvis are formed. The female pelvis is wider and shorter than the male, and the latter is higher and narrower. Wings ilium in the female pelvis are deployed more than in the male. The entrance to the pelvic cavity in women is larger than in men, and has an elliptical shape. The pelvic cavity, cavitas pelvis, resembles a cylinder in women, and a funnel in men. The cape, promontorium, protrudes sharply forward in the male pelvis, and less protrudes forward in the female. The buttocks in women are wide, flat and short, in men they are narrow, high and curved. Ischial tubercles in the female pelvis are more deployed to the sides. The junction of the pubic bones forms an arc, and the lower branches of the ischial and pubic bones form a right angle. In the male pelvis, the pubic branches, combined, form an acute angle.
To predict childbirth and prevent complications great importance have the size and shape of the pelvis.
There are external dimensions of the pelvis, the dimensions of the entrance to the small pelvis and the exit from it: 1) the distance between the two upper anterior spines (spinous distance) of the ilium, distantia spinamm, is 25-27 cm, and between the most distant points of the wings of the ilium, distantia cristarum - 28-30 cm;
2) distance between greater trochanter femur(trochanteric distance), distantia trochanterica - 30-32 cm;
3) the direct diameter [of the conjugate] to the entrance to the small pelvis, or conjugata anatomica, is the distance between the promontory and the upper edge of the pubic symphysis and is equal to 11 cm;
4) transverse diameter, diameter transversa (the distance between the most distant points of the boundary line in the frontal plane) is 13 cm;
5) oblique diameter, diameter obliqua (the distance between the sacroiliac joints on one side and the iliac-pubic eminence on the second) is 12 cm;
6) the direct size, diameter recta, of the exit from the pelvic cavity in women (the distance between the tip of the coccyx and the lower edge of the pubic symphysis, which depends on the degree of mobility of the coccyx) is 9-12 cm;
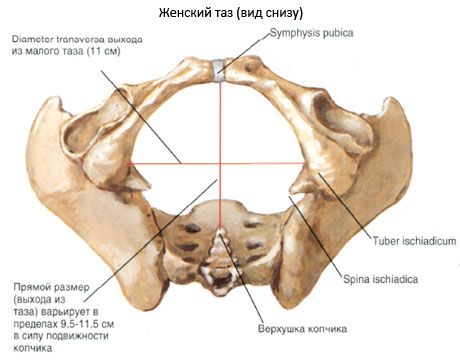
7) the transverse size, diameter transversa, of the exit from the pelvic cavity (the distance between the inner edges of the ischial tubercles) is 11 cm.
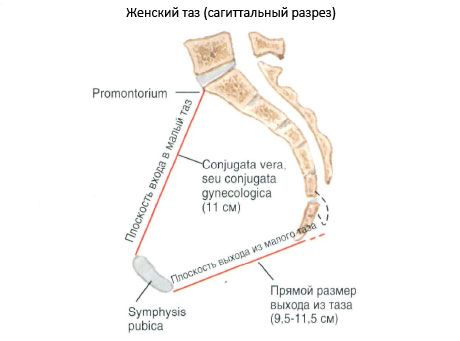
AT obstetric practice it is important to know the smallest anteroposterior dimension in the area pelvic inlet. This size is the real conjugate, conjugata vera - the distance between the cape and the surface of the bottom fusion most protruding into the pelvic cavity. It is also called gynecological conjugate, conjugata gynaecologica, which indicates its practical significance. The size of the true conjugate of the female pelvis is on average 10.5-11 cm.
The male pelvis is 1.5-2 cm smaller than the female one. Deviations from the size of the pelvis depend on age, type of body posture, and the size of the subject. Individual characteristics outward difference the pelvis may touch the shape and size of the sacrum, pelvic bones and the degree of expression of the cape.
Negative influence on the shape of the pelvis various diseases: rickets, spinal deformity and natural malformations.
X-ray anatomy. Radiography of the pelvic bones is carried out in three projections: posterior, direct and lateral. In the pictures in the rear projection, all parts of the pelvic bone, the triangular shape of the buttocks, the entrance to the pelvis, the obturator foramen and the gap of the hip joint are clearly defined. In the middle between the pubic bones there is an enlightenment corresponding to the discus interpubicus - this is the X-ray slit of the pubic symphysis.
The pelvis (pelvis) is formed by the connecting pelvic bones and the sacrum. It is a bone ring. The pelvis is a container for many internal organs. With the help of the pelvic bones, the trunk is connected with the lower limbs. There are two departments - a large and small pelvis.
The large pelvis (pelvis major) is delimited from the lower pelvis by a boundary line. The border line (linea terminalis) passes through the cape of the sacrum, along the arcuate lines of the ilium, crests of the pubic bones and the upper edge of the pubic symphysis. The large pelvis is bounded behind by the body of the V lumbar vertebra, from the sides by the wings of the ilium. Large pelvis in front bone wall does not have.
The small pelvis (pelvis minor) is bounded behind by the pelvic surface of the sacrum and the ventral surface of the coccyx. Laterally, the walls of the pelvis are the inner surface of the pelvic bones (below the border line), sacro-spinous and sacro-tuberous ligaments. The anterior wall of the small pelvis is the upper and lower branches of the pubic bones, the pubic symphysis.
The small pelvis has an inlet and outlet. The upper aperture (hole) of the pelvis (apertura pelvis superior) is limited by the boundary line. The exit from the small pelvis - the lower aperture of the pelvis (apertura pelvis inferior) is limited from behind by the coccyx, from the sides by the sacrotuberous ligaments, branches of the ischial bones, ischial tubercles, lower branches of the pubic bones, and in front - by the pubic symphysis. The obturator opening located in the side walls of the small pelvis is closed by a fibrous obturator membrane (membrana obturatoria). Throwing through the obturator groove, the membrane limits the obturator canal (canalis obturatorius). Vessels and a nerve pass through it from the pelvic cavity to the thigh. In the side walls of the small pelvis there are also large and small sciatic foramen. The large sciatic foramen (foramen ischiadicum majus) is limited by the large sciatic notch and the sacrospinous ligament. The small sciatic foramen (foramen ischiadicum minus) is formed by the small sciatic notch, sacro-tuberous and sacrospinous ligaments.
The structure of the pelvis is associated with the gender of a person. The upper aperture of the pelvis vertical position body in women forms an angle of 55-60 ° with the horizontal plane. The pelvis in women is lower and wider, the sacrum is wider and shorter than in men. The cape of the sacrum in women protrudes less. Ischial tubercles are more deployed to the sides, the distance between them is greater than in men. The angle of convergence of the lower branches of the pubic bones in women is 90° (pubic arch), in men it is 70-75° (subpubic angle).
For forecasting birth process it is important to know the size of a woman's pelvis. Practical value have the size of both small and large pelvis. The distance between the two upper and anterior iliac spines (distantia spinarum) in women is 25-27 cm. The distance between the most distant points of the wings of the ilium (distantia cristarum) is 28-30 cm.
The direct size of the entrance to the small pelvis (true, or gynecological, conjugate - conjugata vera, s. gynaecologica) is measured between the cape of the sacrum and the most posterior point of the pubic symphysis. This size is 11 cm.
The transverse diameter (diameter transversa) of the entrance to the small pelvis - the distance between the most distant points of the boundary line - is 13 cm.
The oblique diameter (diameter obliqua) of the entrance to the small pelvis is 12 cm. It is measured between the sacroiliac joint of one side of the pelvis and the iliopubic eminence of the other side.
In men and women, the pelvis forms a bony ring through which body weight is distributed to lower limbs, but in women, the pelvis has some features that are adapted for childbearing. The pelvis is made up of four bones: the sacrum, the coccyx, and two pelvic or innominate bones. The pelvic bones are attached to the sacrum with the help of the sacroiliac synchondroses and to each other with the help of the pubic symphysis.
Pelvic bone
Each pelvic bone is formed by the fusion of the ilium, ischium, and pubic bones. Connecting with each other, these bones form the acetabulum.
The ilium has an upper section - a wing and a lower section - a body. The place of their connection has an arcuate shape - an arcuate line. There are several protrusions on the wing of the ilium: in front - the anterior superior iliac spine, slightly below it - the anterior inferior iliac spine; behind - the posterior superior iliac spine and the posterior inferior iliac spine.
It makes up the lower and posterior third of the pelvic bone. It has a body that is involved in the formation of the acetabulum, and branches. The body and the branch form an angle between themselves, at the top of which is a thickening - the ischial tuberosity. The branch of the ischium joins the inferior branch of the pubic bone. On the back surface, the branch of the ischium has a protrusion - the ischial spine. The ischium participates in the formation of the lesser ischial notch.
Pubic bone forms the anterior wall of the pelvis and consists of a body and two branches: the upper, horizontal and lower, descending. The lower branches of the pubic bones form an angle - the pubic arch. The body of the pubic bone is involved in the formation of the acetabulum. In the place of conjugation of the ilium and pubic bones is the iliopubic elevation. Along the top edge top branch pubic bone passes a bone crest, ending with a pubic tubercle. Both pubic bones are attached to each other with the help of the pubic symphysis. The pubic symphysis inside has a cavity that is filled with fluid and increases during. Relaxation of the symphysis begins in the first half of pregnancy and is especially pronounced during the last 3 months. The regression of such relaxation begins immediately after childbirth and is completely completed after 3-5 months.
The sacrum consists of 5-6 fixedly interconnected vertebrae and has a uniformly concave anterior surface. The first vertebra of the sacral bone is connected with the fifth with the help of cartilage. lumbar vertebra, forming a ledge - cape. The sacrum is connected to each of the pelvic bones with the help of flat cartilaginous sacroiliac joints, which have some mobility, and two ligaments: sacro-awn and sacro-hump.
The sacro-ostevaya ligament runs from the posterior surface of the sacrum to the ischial spine, the sacro-hump ligament - from the posterior surface of the sacrum to the ischial tuberosity. These ligaments go around the small and large sacrosciatic notches and form a large and small sciatic foramen.
The coccygeal bone is usually formed by 4-5 fused vertebrae, joins the distal end of the sacrum with the help of a movable crion-coccygeal joint. During childbirth, thanks to this joint, the coccyx can deviate by 1-1.5 cm.
pelvic floor(perineum) is a group of fascia and muscles that supports the pelvic organs and is localized in the area between the thighs from the coccyx to the pubic bone. The perineum is bounded in front by the pubic symphysis, on the sides by the ischial tuberosities, and in the back by the coccyx. bottom surface the anus lift muscle forms upper bound perineum. The floor of the perineum consists of the skin and two layers of superficial fascia - the superficial subcutaneous fat layer (Camper's fascia) and the deep membranous layer (Collis's fascia). A transverse line drawn through the center of the perineum divides it into anterior and posterior parts, or triangles - the urogenital (urogenital diaphragm) and anal triangles (pelvic diaphragm).
pelvic diaphragm(anal triangle) is wide but thin muscle layer, which forms lower bound abdominal (and pelvic) cavity and consists of a wide funnel-shaped belt of fascia and muscles, extending from the symphysis to between the walls of the pelvis. The pelvic diaphragm consists of 3 groups of muscles and fascia that cover:
- Anus lift muscles;
- coccygeal muscle;
- External anal sphincter.
These structures are the evolved remnants of the tail muscles of lower animals. The anus levator muscle is the longest and strongest of all muscles and forms a wide muscular belt extending from the posterior surface of the superior ramus of the pubis, inner surface ischium and between these two formations from the obturator fascia. Muscle fibers are distributed in several directions: in the urethra, vagina and rectum, forming functional fibers around them. The anus lift muscle is divided into three paired components, which are named according to their anatomical location: the pubococcygeal, ischiorectal, and iliococcygeal muscles.
An important space of the pelvic diaphragm is the ischiorectal (ischio-anal) fossa - the space between the skin and the anus lift muscle on both sides anal canal containing adipose tissue bounded by the fascia of Collis. The ischiorectal fossa at the back is combined with the fossa of the same name on the opposite side, forming a "horseshoe".
urogenital diaphragm
The urogenital diaphragm (urogenital triangle) is a strong muscular membrane that occupies the area between the symphysis and ischial tuberosities and passes through the triangular anterior part of the pelvic outlet. The urogenital diaphragm is located outside and below the pelvic diaphragm and is formed by two spaces, or layers: superficial and deep.
The superficial space of the perineum is limited by the deep fascia of the perineum and includes 3 pairs of muscles:
- Ischiocavernosus muscle;
- Bulb-cavernous, or bulbous-spongy muscle;
- Superficial transverse muscle of the perineum.
In this space are the bulbs of the vestibule of the vagina and large vestibules glands (bartholin glands). The ischiocavernosus muscle runs from the medial surface of the ischial tuberosities under the pubic arch to the crura of the clitoris.
The bulbous-cavernous, or bulbous-spongy muscle, which is also called the vaginal sphincter, begins behind the tendinous center of the perineum, passes on both sides of the vestibule of the vagina to the dorsal surface of the clitoris in the lower fascia of the urogenital diaphragm and forms the medial border of the superficial space of the perineum. The superficial transverse perineal muscle runs transversely from the front of the ischial tuberosities to the tendon center of the perineum.
Deep perineal space(triangular ligament) - a closed space between the upper and lower fascia of the urogenital diaphragm, on the sides - the places where this fascia enters the sciatic-pubic branches, which includes the following muscle groups:
- Sphincter urethra;
- Deep transverse muscle of the perineum.
Sphincter of the urethra starts from the pubic-sciatic branches, goes medially to the urethra, covers its distal section, as well as the anterior and posterior walls of the vagina. In women, it is poorly developed due to the fact that it is perforated by two openings: the urethra and the vagina.
Deep transverse perineal muscle consists of transverse muscle fibers that run along the posterior face of the urethral sphincter and enter the central tendon center of the perineum. Unlike men, in women this muscle plays a very minor role in the mechanism of urinary retention.
The blood supply to the perineum is carried out by the internal pudendal artery and its branches: the lower rectal and posterior labial arteries.
The innervation of the perineum occurs due to the pudendal nerve (from the second, third and fourth sacral segments) and its branches.
Clinical correlations
The ischial spines are of great obstetric importance, since the distance between them is usually equal to the smallest diameter of the pelvic cavity. They are also a landmark for the advancement of the presenting part of the fetus along the axis of the birth canal. When a woman is in a dorsal lithotomy position during childbirth, due to the mobility of the sacroiliac joints, the diameter of the pelvic outlet can increase by 1.5–2 cm. This circumstance is the main argument for placing a woman in such a position during childbirth.
All layers of the muscles of the perineum during childbirth form a wide muscular canal, which is a continuation of the bone birth canal. The paired anus lift muscle has importance to maintain abdominal and pelvic organs, distribution intra-abdominal pressure along with the diaphragm and muscles abdominal wall(for example, with), control of the content of urine and feces, as well as for the process of childbirth (significant stretching of the tile-like muscle fibers as the fetus advances, followed by their contraction). With the contraction of this muscle, the genital slit, rectum and vagina are compressed.
The presence of adipose tissue in the ischiorectal fossa facilitates stretching of the anal canal during defecation and the vaginal canal during the second stage of labor. It can become a place of accumulation of blood when postpartum hemorrhage(hematoma) or pus in abscesses and can hold up to 1 liter of fluid. Such abscesses can move to the opposite side of the pelvis.
The female pelvis in obstetrics
The bone pelvis creates a solid foundation for the soft tissues of the birth canal and determines its direction and size. The bones of the female pelvis are thinner, the plane of the entrance to the small pelvis usually has the shape of a transversely narrowed oval, while the plane of the entrance of the male pelvis is funnel-shaped. The female pelvis is lower, wider and more capacious than the male; the pubic symphysis is shorter. The cavity of the female pelvis becomes wider towards the exit due to the flatness of the ilium, the greater distance between the ischial tuberosities, and the greater subpubic angle (90-100° compared to 70-75° in men).
From an obstetric point of view female pelvis divided into two parts. The boundary between them is the boundary line. It runs along the inner surface of each ilium from the sacroiliac joint in the iliopubic eminence and divides the pelvis into two parts: the upper (large pelvis) and the lower (small, or real pelvis).
The large pelvis cannot serve as a guide to the capacity of the small pelvis, but it is easily accessible for measurement, and therefore some of its dimensions are used for an approximate assessment of the size of the small pelvis:
- Interosseous distance - the distance between the anterior superior iliac spines (25-26 cm);
- Intercrest distance - the distance between the most distant points of the iliac crests (28-29 cm);
- Inter-acetabular distance - the distance between the most distant points hip joints(30-31 cm);
- The external conjugate is the Bodelok conjugate, the external obstetric conjugate is the distance from the fossa between the spinous processes of the last lumbar and first sacral vertebra to the most protruding point of the symphysis (20-21 cm).
Small(real) pelvis
He has highest value for childbearing. It is bounded from above by the cape of the sacrum, the border line and the upper edge of the pubic bones, from below by the exit of the pelvis. The anterior wall in the region of the symphysis is about 5 cm long, the posterior (in the region of the sacrum) is about 10-12 cm. The lateral walls of the small pelvis are represented by the internal surfaces of the ischial bones. When the woman is upright top part the pelvic canal is directed down and back, and the lower one forms an arc and goes down and forward. Lateral walls of the small pelvis adult woman have a somewhat convergent direction. The descending branches of the pubic bones in the normal female pelvis form a circular arc (subpubic angle 90-100°), which allows passage of the fetal head.
In the small pelvis, 4 conditional planes are distinguished, they help to navigate in determining the localization of the presenting part of the fetus during childbirth:
The plane of entry into the small pelvis;
The plane of the wide part of the pelvic cavity (passes through the largest diameter of the pelvis);
The plane of the narrow part of the pelvic cavity (passes through the small diameter of the pelvis);
The plane of the exit of the small pelvis.
The plane of entry into the small pelvis is limited behind the cape and wings of the sacrum; on the sides - by the border line, in front - by the symphysis and upper (horizontal) branches of the pubic bones. The configuration of the entrance to the female pelvis in 50% of women is more rounded than oval (gynecoid type of the pelvis). In the plane of the entrance to the small pelvis, 4 diameters have obstetric significance: straight (anteroposterior, real conjugate), transverse and two oblique.
Straightdiameter- real conjugate (internal obstetric conjugate) - the most important anteroposterior diameter, which is the smallest distance between the cape and the inner upper edge (10-11 cm). The distance between the cape of the sacrum and the upper edge of the symphysis (anteroposterior diameter of the anterior opening of the pelvis) is called the anatomical conjugate and is equal to 11.5 cm.
Transversediameter- the distance between the most distant points of the intermediate line (13-13.5 cm).
obliquediameter- the distance between the sacroiliac joint on one side and the iliopubic eminence on the opposite side (12-12.5 cm). The right diameter is measured from the right sacroiliac joint, the left one from the left.
The plane of the wide part of the cavity of the small pelvis is limited in front by the middle of the inner surface of the symphysis, from the sides - by the middle of the hip cavities, behind - by the message of the II and III sacral vertebrae. In the wide part of the small pelvis, a straight (12.5 cm) and transverse (12.5 cm) diameter is determined.
The plane of the narrow part of the cavity of the small pelvis is limited in front by the lower edge of the pubic symphysis, on the sides - by the awns of the ischial bones, and behind - by the sacrococcygeal joint. In this plane, straight (11.5 cm) and transverse (10.5 cm) diameters are also distinguished.
The plane of the exit of the small pelvis is limited in front by the lower edge of the pubic arch, on the sides - by the ischial tubercles, and in the back - by the tip of the coccyx. It has a straight diameter of 9.5 cm, but if the coccyx deviates, it can increase by 1.5-2 cm and equals 11-11.5 cm; and a transverse diameter (between ischial tuberosities), which is 11 cm (not less than 8 cm). In the plane of the exit of the pelvis, an anus sagittal diameter is also distinguished (a segment of a straight diameter from the top of the coccyx to the point of intersection with the transverse diameter), which in normal pelvis should not be less than 7.5 cm. vaginal delivery depends on the size of the anus sagittal diameter.
So, in the plane of the entrance to the pelvis, the transverse diameter is the largest; in the wide part of the pelvic cavity, the direct and transverse diameters are the same (this plane has no special obstetric significance); in the narrow part of the cavity of the small pelvis and in the exit plane, the straight diameters are the largest. These provisions are important for understanding the biomechanism of labor in a normal pelvis.
Pelvicaxis, or leading line of the pelvis, connecting the midpoints of the direct diameters of all planes of the small pelvis and is directed down and back at the entrance to the pelvis, down and forward at the exit.
The angle of inclination of the pelvis is formed between the plane of the entrance to the pelvis and the horizontal line with the vertical position of the woman and is 45-60 ° (in non-pregnant women- 45-46°).
Classification of pelvic types
A line drawn through the transverse diameter of the plane of entry into the pelvis divides it into anterior and posterior segments. The shape of these segments is taken into account when classifying the types of the pelvis. So, the nature of the posterior segment determines the type of pelvis, the anterior - a tendency that helps to identify mixed types pelvis.
Gynecoid pelvis. The posterior sagittal diameter is slightly less than the anterior sagittal diameter, the sides of the posterior segment are rounded and wide. Given that the transverse diameter of the entrance to the pelvis is almost the same as the anteroposterior one, the entrance to the pelvis has almost round shape or oval. The pelvic walls are straight, the ischial spines do not protrude and the distance between them exceeds 10 cm. The pubic arch is wide.
The sacrosciatic notch is rounded. The sacrum is not deflected either anteriorly or posteriorly. It occurs in 50% of women and has best forecast by vaginal delivery.
The anthropoid pelvis differs in that the direct diameter of the entrance to the pelvis exceeds the transverse one, therefore the shape of the entrance to the pelvis has the form of an oval, narrowed in the anteroposterior direction. The anterior segment is narrow. The sacrosciatic notch is wide, the pelvic walls converge somewhat. The sacrum is usually straight and has 6 vertebrae, making the anthropoid pelvis the deepest of all pelvic types. The ischial spines protrude somewhat. The subpubic arch is well defined, but may be somewhat narrowed. This type of pelvis occurs in 25% of women of the white race and about 50% in representatives of other races.
androidpelvis. The posterior sagittal diameter of the entry is significantly shorter than the anterior sagittal diameter, which limits the space for the fetal head. The walls of the posterior segment are not round and approach wedge-shaped. The anterior segment is narrow and triangular. The lateral walls of the pelvis tend to converge, the ischial spines protrude, the subpubic arch is narrowed. The sacro-ischial notch is narrow. The sacrum protrudes somewhat into the pelvis and is of course straight, with an unexpressed depression. The posterior sagittal diameter decreases from the entrance to the exit of the pelvis due to the protrusion of the sacrum. May occur in 30% of women. A narrowed android pelvis has a poor prognosis for vaginal delivery.
Platypeloidpelvis- the pelvis, which has a flattened gynecoid shape, with a short anteroposterior (straight and wide transverse) diameter. The angle of the anterior segment is very wide, the arcs of the anterior and posterior segments correct form. The sacrum is short, the sacrosciatic notches are wide. This type of pelvis is less common (in 3% of women).
Clinical determination of pelvic capacity
Diagonalconjugate
In many narrowed straight (anteroposterior) pelvises, the diameter of the pelvic inlet is reduced. To predict childbirth, it is important to determine this size, but this is possible only with a special instrumental research(X-ray pelvimetry, nuclear magnetic resonance and computer pelvimetry, ultrasonic pelvimetry). But the distance between the lower edge of the pubic symphysis and the cape of the sacrum (diagonal conjugate) can be determined during a gynecological examination.
When determining the diagnonal conjugate, the doctor inserts two fingers into the vagina, determines the mobility of the coccyx and the nature of the anterior surface of the sacrum (vertical and lateral arcs). In a normal pelvis, only the last three can be palpated sacral vertebrae, while in the narrowed pelvis the entire surface of the sacrum is available for palpation. If the size of the diagonal conjugate exceeds 11.5 cm, the capacity of the pelvis is considered sufficient for vaginal delivery, provided normal sizes fetus.
transverseconstriction of the pelvis(this type of narrowing of the pelvis can be observed with a normal anteroposterior diameter) can only be detected when special study(X-ray pelvimetry, nuclear magnetic resonance and computer pelvimetry, ultrasonic pelvimetry). With ultrasound pelvimetry, it is possible to determine the real conjugate, the dimensions of the planes of the small pelvis, biparietal size fetal head, its location and insertion, expected fetal weight.
The large pelvis is much wider than the small one, it is bounded laterally by the wings of the ilium, behind by the last lumbar vertebrae, and in front by the lower abdominal wall. The volume of the large pelvis can change in accordance with the contraction or relaxation of the abdominal muscles. The large pelvis is available for research, its dimensions are determined and quite accurately. By the size of the large pelvis, the size of the small pelvis is judged, which is not available for direct measurement. Meanwhile, determining the size of the small pelvis is important, since the fetus passes through the unyielding bone canal of the small pelvis.
Small pelvis
Planes and dimensions of the small pelvis. The small pelvis is the bony part of the birth canal. Back wall The small pelvis consists of the sacrum and the coccyx, the lateral ones are formed by the ischial bones, the anterior - by the pubic bones and symphysis. The posterior wall of the small pelvis is 3 times longer than the anterior one. Upper section The small pelvis is a solid, unyielding bone ring. AT lower section the walls of the small pelvis are not continuous; they have obturator openings and ischial notches, limited by two pairs of ligaments (sacrospinous and sacrotuberous).
In the pelvis, there are the following departments: entrance, cavity and exit. In the pelvic cavity there are wide and narrow part. In accordance with this, four planes of the small pelvis are considered: I - the plane of the entrance to the pelvis, II - the plane of the wide part of the cavity of the small pelvis, III - the plane of the narrow part of the pelvic cavity, IV - the plane of the exit of the pelvis.
/. The plane of the entrance to the small pelvis has the following boundaries: in front - the upper edge of the symphysis and the upper inner edge of the pubic bones, from the sides - nameless lines, behind - the sacral cape. The entrance plane has the shape of a kidney or a transverse oval with a notch corresponding to the sacral promontory. At the entrance to the pelvis, three sizes are distinguished: straight, transverse and two oblique.
- Straight size - the distance from the sacral cape to the most prominent point on the inner surface of the pubic symphysis. This size is called obstetric, or true, conjugate (conjugata vera). There is also an anatomical conjugate - the distance from the cape to the middle of the upper inner edge of the symphysis; the anatomical conjugate is slightly (0.3-0.5 cm) larger than the obstetric conjugate. Obstetric, or true conjugate is equal to 1 1 cm
- Transverse dimension - the distance between the most distant points of the nameless lines. This size is 13-13.5 cm.
oblique dimensions two: right and left, which are equal to 12-12.5 cm. Right oblique size - distance from the right sacroiliac joint to the left iliac-pubic tubercle, left oblique dimension- from the left sacroiliac joint to the right iliac-pubic tubercle. In order to make it easier to navigate in the direction of the oblique dimensions of the pelvis in a woman in labor, M.S. Malinovsky and M.G. Kushnir offer the following reception. The hands of both hands are folded at a right angle, with the palms facing up; the ends of the fingers are brought closer to the outlet of the pelvis of the lying woman. The plane of the left hand will coincide with the left oblique size of the pelvis, the plane of the right hand with the right.
II. The plane of the wide part of the pelvic cavity has the following boundaries: in front - the middle of the inner surface of the symphysis, on the sides - the middle of the acetabulum, behind - the junction of the II and III sacral vertebrae. In the wide part of the pelvic cavity, two sizes are distinguished: straight and transverse.
- Straight the size - from the junction of II and III sacral vertebrae to the middle of the inner surface of the symphysis; equal to 12.5 cm.
- Transverse the size - between the tops of the acetabulum; equal to 12.5 cm.
There are no oblique dimensions in the wide part of the pelvic cavity because in this place the pelvis does not form a continuous bone ring. Oblique dimensions in the wide part of the pelvis are allowed conditionally (length 13 cm).
///. The plane of the narrow part of the pelvic cavity bounded in front by the lower edge of the symphysis, laterally by the awns of the ischial bones, behind by the sacrococcygeal articulation. There are two sizes: straight and transverse.
- Straight the size goes from the sacrococcygeal joint to the lower edge of the symphysis (apex of the pubic arch); equals 11-11,5 cm.
- Transverse dimension connects the awns ischium; equal to 10.5 cm.
IV. Pelvic outlet plane has the following boundaries: in front - the lower edge of the symphysis, from the sides - ischial tubercles, behind - the tip of the coccyx. The pelvic outlet plane consists of two triangular planes, common ground which is the line connecting the ischial tuberosities. In the outlet of the pelvis, two sizes are distinguished: straight and transverse.
- Direct pelvic outlet size goes from the top of the coccyx to the lower edge of the symphysis; it is equal to 9.5 cm. When the fetus passes through the small pelvis, the coccyx departs by 1.5-2 cm and the direct size increases to 1 1.5 cm.
- Transverse dimension of the pelvic outlet connects the inner surfaces of the ischial tubercles; is 11 cm. Thus, at the entrance to the small pelvis, the largest size is the transverse one. In the wide part of the cavity, straight and transverse dimensions are equal; the largest size will be the conditionally accepted oblique size. In the narrow part of the cavity and the outlet of the pelvis, the direct dimensions are larger than the transverse ones.
In addition to the above (classical) cavities of the pelvis, there are parallel planes of the pelvis (planes goji).
The first (upper) plane passes through the terminal line (I. terminalis innominata) and is called therefore terminal plane.
Second - main plane runs parallel to the first at the level of the lower edge of the symphysis. It is called the main one because the head, having passed this plane, does not encounter significant obstacles, since it has passed a continuous bone ring.
Third - spinal plane, parallel to the first and second, crosses the pelvis in the spina oss. ischii.
Fourth - exit plane, represents the bottom of the small pelvis (its diaphragm) and almost coincides with the direction of the coccyx.
The wire axis (line) of the pelvis. All planes (classical) of the small pelvis border in front with one or another point of the symphysis, and behind - with different points of the sacrum or coccyx. The symphysis is much shorter than the sacrum with the coccyx, so the planes of the pelvis converge in an anterior direction and fan-shaped diverge backwards. If you connect the middle of the direct dimensions of all the planes of the pelvis, you will get not a straight line, but a concave anterior (to the symphysis) line. This conditional line connecting the centers of all direct dimensions of the pelvis is called wire axis of the pelvis. The wire axis of the pelvis is initially straight, it bends in the pelvic cavity in accordance with the concavity of the inner surface of the sacrum. In the direction of the wire axis of the pelvis, the fetus passes through the birth canal.
Pelvic tilt angle(the intersection of the plane of its entrance with the plane of the horizon) when a woman is standing, it can be different depending on the physique and ranges from 45-55 °. It can be reduced if the woman lying on her back is forced to pull the hips strongly to the stomach, which leads to the elevation of the womb. It can be increased by placing a roll-shaped hard pillow under the lower back, which will lead to the downward deviation of the womb. A decrease in the angle of inclination of the pelvis is also achieved if the woman is given a semi-sitting position, squatting.
