Congenital defects and anomalies. Birth defects: causes, prevention and treatment
Some of the birth defects presented below are quite well known, while others are extremely rare. But be that as it may, they are all quite creepy, mysterious and tragic. So…
This is a rare condition (approximately one in 200,000 births) in which twins are born joined in one or more parts of the body. In 70–75% of all cases, conjoined twins are female. About half are stillborn. Sometimes they can be separated, which allows Siamese twins live full life, but more often than not, this is impossible.
Hypertrichosis (Ambrams syndrome)

Hypertrichosis is a disease manifested in excess growth hair unusual for this area of skin. Fortunately, it is very important, and currently there are only 40 people in the world suffering from hypertrichosis. The disease is extremely debilitating for children as they are often rejected by their peers.
Sirenomelia (mermaid syndrome)

Sirenomelia is a developmental anomaly manifested as a fusion lower limbs. Occurs in one case per 100 thousand newborns. As a rule, it leads to death 1–2 days after birth, this is due to strange development and functioning of the kidneys and Bladder. However, there are cases where children with this anomaly (even without surgical intervention) lived for several years. Thus, the American girl Shiloh Pepin, who suffered from sirenomelia, was able to live for more than 10 years.

Cyclopia, as you might guess, is named after the famous mythical creature Cyclops. Children born with cyclopia have only one eye, located in the middle of the head. In 100% of all cases, newborns die in the first days of life.
A type of twin fusion in which the head normal child the twin's head grows in without a body. History knows only ten recorded examples of this anomaly, and only in three of them the child remained alive after birth. In one case, the second head was able to smile, blink, cry, and suckle at its mother's breast.
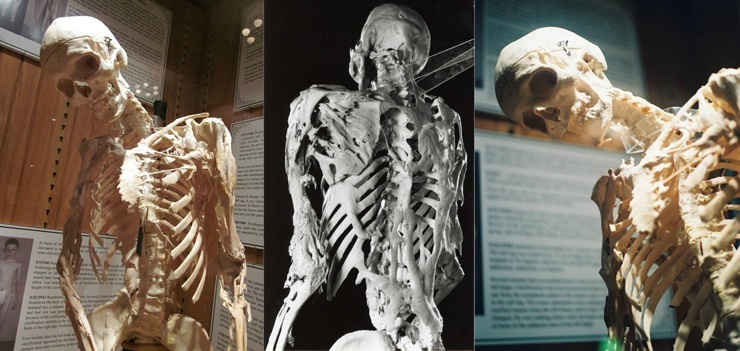
Rare disease(1 case in 2 million), resulting as a result of a gene mutation and manifested by congenital developmental defects - primarily curved ones thumbs stop and disorders in cervical spine spine. The basis of fibrodysplasia is the formation inflammatory processes in tendons, ligaments, fascia, aponeuroses and muscles, which in end result leads to their calcification and ossification. The disease is also called “Disease of the Second Skeleton”, since, in fact, where normal anti-inflammatory processes are required to occur in the body, bone growth begins.

Progeria - the rarest genetic defect, in which skin changes occur and internal organs, conditioned early aging body. No more than 80 cases of progeria have been recorded in the world.

Birth defect, in which the baby is born with a semi-functional tail complete with muscles, nerves, skin and blood vessels. It is believed that it may be caused by a gene mutation.

Anencephaly - complete or partial absence cerebral hemispheres brain, calvarial bones and soft tissues. Occurs approximately once in 10 thousand newborns (in the USA), more often in female fetuses. The defect is fatal in 100% of cases. 50% of fetuses with anencephaly die in utero, the remaining 50% are born alive, but only 66% can survive for several hours (however, some have been known to live for about a week). Stephanie Keene, better known by her nickname Baby Kay, is considered the “longest-liver” among anencephalics, who lived with this terrible diagnosis for 2 years and 174 days.
Share on social media networks
Approximately 2-3% of newborns have serious congenital malformations. Embryologically, such defects are classified into three main classes (Table 36-6):
Birth defects as a result of incomplete morphogenesis;
Birth defects resulting from repetitive morphogenesis;
Birth defects resulting from aberrant morphogenesis. Incomplete morphogenesis is the most common pathology, aberrant - the rarest.
Table 36-6.
(Cohen M.M., 1997)
Almost all congenital malformations occur in embryonic period(3-10th week of gestation), during the period when organ differentiation occurs (Table 36-7).
Congenital defects can be simple or complex. How later date the occurrence of a congenital defect, the more likely that there will be no pathogenetically associated defects in nearby embryonic structures (simple congenital malformations). If the defect occurs in the early stages of embryogenesis, the probability of involvement of nearby structures is quite high, and a cascade of multiple birth defects development or sequence (sequence) of congenital malformations. An example is the Pierre Robin sequence, when the primary defect is intrauterine hypoplasia lower jaw causes a disruption in the process of tongue retraction, which, in turn, leads to cleft palate.
Table 36-7. Time of formation of congenital malformations (Cohen M.M., 1997)
Congenital malformation in its clinical manifestation can be minimal (bifurcation of the uvula) and maximally pronounced (cleft palate). In the case of minimal manifestation, it will be defined as minor anomaly development. A complex malformation or sequence may also present with minimal clinical version.
For example, the sequence of holoprosencephaly in its most severe version is characterized by a congenital malformation of the cerebral hemispheres and facial anomalies - absence of nasal structures, hypotelorism, premaxillary agenesis with cleft lip and alveolar process upper jaw; in its minimal clinical form, it is characterized by a combination of hypotelorism with a single maxillary incisor. Knowing this is extremely important for the family genetic prognosis of a child with holoprosencephaly - examining the parents for minimal clinical manifestations.
DEFORMATION
This type of birth defect occurs in approximately 1-2% of newborns. The most common defects are clubfoot, congenital hip dislocation and postural scoliosis. Deformations most often occur in the late fetal period as a result of the influence of three main causes and predisposing factors (Table 36-8): mechanical causes; congenital malformations; functional reasons.
Mechanical causes of deformities are the most common and occur against the background of fetal hypokinesia. In a study of 4,500 newborns, it was shown that among all newborns with deformities, 1/3 of children had two or more deformities. This sequence congenital deformities is well illustrated by an example where uterine rigidity is the cause of three deformities - plagiocephaly, asymmetry of the lower jaw and clubfoot in one newborn.
Table 36-8. Predisposing factors in the development of deformities (Cohen M.M., 1997)
| Mechanical | |
| causes | Rigidity of the uterus and abdominal muscles (combined with |
| first birth) | |
| Short stature and reduced body size in a pregnant woman | |
| women | |
| Hypoplasia pelvic ring | |
| Hypoplasia of the uterus | |
| Bicornuate uterus | |
| Leiomyoma of the uterus | |
| Unusual implantation site | |
| Chronic leakage of amniotic fluid | |
| Low water ( of various etiologies) | |
| Unusual fetal position | |
| Early pelvic insertion of the fetal head | |
| Multiple pregnancy | |
| Congenital malformations of the fetus | |
| Big fruit(congenital macrosomia) | |
| Macrocephaly or fetal hydrocephalus | |
| Congenital defects | Spina bifida; |
| fetal development as | |
| cause of deformation | Other congenital malformations nervous system fetus |
| Fetal renal agenesis (bilateral) | |
| Severe renal hypoplasia | |
| Severe polycystic kidney disease | |
| Urethral atresia | |
| Functional | Neurological disorders(congenital hypotension) |
| causes | |
| Muscle disorders | |
| Defects connective tissue | |
Almost all severe birth defects urinary system cause oligohydramnios, which, in turn, causes Potter's syndrome (unusual fetal face, multiple contractures of the limbs).
Functional causes of deformities include various shapes congenital hypotonia of newborns and neuromuscular types of arthrogryposis. Congenital hypotonia can be combined with micrognathia, microglossia, and prominent lateral sutures hard palate, abnormal flexion folds of the hand and foot, flat-valgus feet and other deformities. Arthrogryposis is characterized by congenital rigidity of the limbs and fixation of the joints in a characteristic position.
DISRUPTION
The exact frequency of disruption is unknown; it is detected in 1-2% of newborns. The first researcher to describe this type pathology in the 1968 monograph “Fetal Malformations Caused by Amnion Rupture During Gestation”, was R. Torpin (Cohen M.M., 1997). Disruptions arise as a result of exposure various reasons: vascular factors, anoxia, infections, radiation, teratogens, amniotic cords, mechanical factors. The type and severity of disruption depend on the duration of pregnancy, the location of exposure and the degree of tissue damage. Most often, disruptions occur during the fetal period, but teratogenic effects are characteristic of embryonic morphogenesis. Some of these effects that occur during the embryonic period “phenocopy” congenital malformations. For example, amniotic cords early date Pregnancies can cause anencephaly, cleft lip and palate, and reduction defects of the limbs. Most difficult differential diagnosis between a congenital malformation and disruption as a result of vascular pathology (Table 36-9).
Table 36-9. Mechanisms of vascular disruption in the embryo and fetus (Cohen M.M., 1997)
| Pathogenesis | Structural anomaly |
| Destruction of the embryonic capillary network | Early amniotic sequence, limb-torso wall complex, reduction anomalies of the limbs, hypoplasia of the maxillary region and limb |
| Persistence of embryonic vessels | Limb defects: radial aplasia, tibial aplasia, fibular aplasia, clubfoot |
| Premature amputation of embryonic vessels | Pathology sequence subclavian artery(Poland, Mobius, Klippel-Feil sequences), gastroschisis, horseshoe kidney |
| Impaired vascular maturation | Capillary hemangiomas, arteriovenous fistulas, aneurysms (Berry aneurysms) |
| Occlusion (external compression) of blood vessels | Anomalies associated with leiomyomas, with tubal pregnancy and bicornuate uterus |
| Occlusion (embolic thrombosis) of blood vessels | Porencephaly, hydranencephaly, microcephaly, gallbladder atresia, distal syndactyly, hemifacial microsomia (rare), bilateral anorchism, cutaneous aplasia |
| Hemodynamic disturbance | Abnormalities Caused by Cocaine Use During Pregnancy |
Isolated congenital developmental defects do not cause difficulties in diagnosis. A completely different situation is observed in the field of multiple congenital developmental defects, where empirical experience and knowledge about the diagnosis and treatment of children with isolated congenital defects is not only insufficient, but often erroneous.
The needs of clinical practice have contributed to the expansion of research efforts to study the etiology and pathogenesis of multiple congenital developmental defects. This section was later called syndromology. One of the clear illustrations of the difference between syndromology and classical medicine, i.e. medicine, where isolated pathology of one organ or system is diagnosed and studied, is the fact that in classical medicine During the 20th century, only a few new diseases were described ( radiation sickness, Legionnaires' disease, AIDS, Lyme disease), while in syndromology the number of such nosological forms has exceeded 5000 and at least 80 new ones are described every year.
For some forms of syndromic pathology, modern molecular genetics has made it possible to localize the genes that determine them and study the products of gene transcription, which are often represented by membrane receptors or tissue growth factors. For example, in Hirschsprung's disease, two mutations of different genes were identified: RET oncogene and endothelin B receptor, which made it possible to distinguish two genetic types of this congenital pathology.
Syndromology is an extremely broad field, covering almost all specialties of medicine. Approximately 1% of all newborns have multiple congenital anomalies or syndromes. Of these, in 40% of cases today it is possible to diagnose a certain syndrome, and the remaining 60% require their identification as “new” syndromes. Although many syndromes are quite rare, the total syndromic forms of pathology constitute a quantitatively significant part of medicine.
Table 36-10. Mechanisms of vascular destruction in the embryo and fetus (Cohen M.M., 1997)
| Environmental factors | Teratogenic effects |
| Pharmacological drugs | |
| Thalidomide | Reduction anomalies of the limbs. Hypoplasia of the upper limb girdle. |
| Ear abnormalities | |
| Alcohol | Delay physical development. Unusual phenotype (short eyes |
| cracks). Microcephaly, mental retardation | |
| DietStyleOestrol | Vaginal adenomatosis. Cervical erosion. Vaginal adenocarcinoma |
| (rarely) | |
| Warfarin | |
| Hypoplasia of nasal cartilage. Congenital defects of the central nervous system. Punctate calcification | |
| epiphyses | |
| Hydantoin (Dilantin) | |
| Delayed physical development. Unusual phenotype. Microcephaly, mental | |
| backwardness | |
| Trirmetadion | |
| Delayed psychomotor development. Unusual phenotype (arched | |
| brows). Cleft lip or palate | |
| Aminopterin | |
| Methotrexate | Spontaneous abortions. Congenital hydrocephalus. Delayed physical development |
| Tia. Unusual phenotype | |
| Streptomycin | |
| Congenital sensorineural hearing loss | |
| Tetracycline | |
| Congenital hypoplasia tooth enamel. Tooth staining (yellow teeth) | |
| Sodium valproate | |
| Neural tube defects (Spina bifida) | |
| Retinol | |
| Spontaneous abortions. Craniofacial anomalies. Neural tube defects | |
| Lithium preparations | |
| Congenital heart defects (Ebstein's anomaly) | |
| Antithyroid drugs | |
| VG. Goiter | |
| Androgens and high doses | |
| masculinizing | Masculinization |
| progestins | |
| Penicillamine | |
| Hyperelastic skin. Congenital pathology connective tissue | |
| Methylmercury (mercury) | Chemical substances |
| Congenital atrophy brain. Spasticity, convulsions. Mental | |
| backwardness | |
| Lead | |
| Delayed physical development. Unusual skin coloration (gray color) | |
| Smoking | Physical, nutritional and other effects |
| Spontaneous abortions. IUGR | |
| Ionizing radiation | |
| The damage depends on the stage of pregnancy. Spontaneous abortions. Congenital | |
| developmental defects (18-36 days of gestation). Microcephaly and mental retardation | |
| Loss (8-15th week of gestation) | |
| Hyperthermia | |
| Congenital defects of the central nervous system | |
| Maternal diabetes mellitus | |
| UPS. Caudal regression syndrome | |
| Iodine deficiency in food | |
| PKU in mother | Goiter. Mental retardation and delayed physical development |
| Abortion, microcephaly, mental retardation |
If the symptoms or symptom complex are caused by one cause (monocausal etiology), then the term syndrome denotes the nosological form of the disease (nosological syndrome) and in this sense is synonymous with the term “disease”. In practice, following the recommendations of international experts, the term “disease” is better used in cases with a progressive course of the disease.
Thus, the syndrome is etiologically certain disease with a pleiotropic (multiple) effect.
An example of such a syndrome is the history of Recklinghausen's disease, or neurofibromatosis type 1. In 1849, Robert Smith, the leading surgeon at Dublin Medical School, published the clinical and pathological features of two cases of neurofibromatosis and cited data from 75 earlier publications in medical literature. However, only in a report by Recklinghausen (von Recklinghausen, 1882) was the idea of neurofibromatosis as a nosological form substantiated. It has now been shown that this pathology is one of the most common hereditary human diseases and occurs with a frequency of 1 in 2000 births. Modern diagnostic criteria of this disease based on such characteristic symptoms, such as skin hyperpigmentation (cafe au lait type), congenital false joints or curvature of the bones of the lower extremities, were developed only in 1987. It should be noted that the diagnosis is possible in cases where the patient has two of the following signs, and provided that they are not symptoms of any other disease.
Diagnostic criteria for neurofibromatosis type 1 (Recklinghausen disease) (WHO memorandum, 1992):
During an examination under artificial light of a patient who has not reached puberty, at least five light brown pigment spots (more than 5 mm at the widest point) are detected; when examining a patient who has reached puberty - at least 6 pigment spots (more than 15 mm at the widest point);
Presence, according to medical history or clinical examination, two or more neurofibromas of any type or one plexiform neurofibroma;
Multiple, freckle-like dark spots in the axillary or groin areas;
Wing dysplasia sphenoid bone or congenital curvature or thinning of long bones with the formation false joint or without it;
Optic nerve glioma;
Two or more Piche's spots/nodules detected on the iris on slit-lamp examination;
The presence of neurofibromatosis type 1, according to the above criteria, in a first-degree relative (parent, sibling or descendant).
Timely diagnosis of Recklinghausen neurofibromatosis requires dynamic observation with periodic CT scans of the head and spinal cord with the aim of early diagnosis neoplasia of the central nervous system.
Already in the 60-70s of the XX century. most chromosomal and teratogenic syndromes have been described and great amount gene syndromes. By the beginning of the 80s of the XX century. experience allowed not only to develop a unified international terminology, but also to propose some methodological approaches for identifying “new” syndromes and studying the pathogenesis of multiple developmental defects (Spranger J. et al, 1982; Cohen MM., 1982; Cohen MM., 1997).
In practice, syndromic forms of pathology also include cases when a child, in addition to any single congenital defect, has an unusual phenotype, that is, the presence of three or more minor developmental anomalies.
Minor developmental anomalies or stigmas of disembryogenesis are abnormal variants of morphology individual organs or fabrics that do not have medical value, i.e. not requiring treatment. The occurrence of these variants is associated with embryonic or, less commonly, with fertile period human morphogenesis. IN clinical genetics and syndromology, minor developmental anomalies are an extremely important diagnostic sign, indicating a high probability serious violations morphogenesis in the form of congenital malformations requiring special diagnostics and often subsequent surgical interventions (Table 36-11).
More than 200 informative morphogenetic variants have been described in humans, although clinical practice Usually no more than 80 minor developmental anomalies are used.
Minor developmental anomalies in newborns:
Head:
V abnormal hair growth pattern;
V flattened occiput;
V “tubercles” of the cranial vault.
Orbital area:
V epicanthic folds;
V epicanthus reverse;
V Mongoloid eye shape;
V anti-Mongoloid eye section;
V short palpebral fissures;
V dystopia of the outer corners of the eye;
V hypotelorism is moderate;
V moderate hypertelorism;
Ptosis is mild;
V heterochromia of the irises;
V microcornea.
Ears:
V primitive form;
V Darwinian tubercle;
V abnormal curl shape;
V asymmetrical ears;
V rotated ears;
V reduced auricles;
V protruding ears;
V absence of a tragus;
Lobe splitting;
V absence of lobe;
V auricular fossae;
V auricular “protrusions”;
V narrowing of the external auditory canal.
Nose and filter:
¦¦¦ hypoplasia of the wings of the nose;
¦¦¦ deployed nostrils;
¦¦¦ flattened filter;
¦¦¦ protruding filter.
Mouth area and oral cavity:
¦¦¦ microgenia;
¦¦¦ splitting of the tongue;
¦¦¦ aberrant frenulum of the vestibule of the mouth;
¦¦¦ neonatal teeth-filter.
¦¦¦ winged neck - moderate;
¦¦¦ neck fistulas.
Vestigial polydactyly; single flexion fold of the palm; abnormal dermatoglyphics; clinodactyly of the little fingers; shortening of the 4th-5th fingers; hypoplasia of the terminal phalanges.
Syndactyly P-Sh fingers; sandal-shaped slits; short 1st finger; fingering (IV-V); thickened nails.
Skin:
Hemangiomas;
Skin hyperpigmentation and nevi; Mongoloid spots (in the white race); skin depigmentation; extra nipples or areolas.
Torso:
¦¦¦ diastasis of the rectus abdominis muscles;
¦¦¦ moderate hypospadias (heads);
¦¦¦ deep impressions of the sacrum.
Skeleton:
¦¦¦ depression or protrusion of the sternum.
The head, neck and hand areas are the most informative regarding these signs; more than 70% of all minor developmental anomalies are located in this area. Diagnostic value minor developmental anomalies are different. It is fundamentally important that the practical significance of these signs lies in the diagnosis of three or more anomalies. Every newborn with three or more minor malformations has a high probability (90%) of a serious congenital malformation of the brain, heart, kidneys or spine, in addition to high probability(50%) diagnosis of the syndromic form of pathology. If a child with a delay in the rate of psychomotor development has three or more minor developmental anomalies, it is stated high risk organic damage CNS (see Table 36-11). Sometimes only the presence of two minor developmental anomalies is informative for diagnosis. For example, hypotelorism (closely located eyeballs) and the only one upper incisor indicate a congenital brain defect of the prosencephalic group type.
Diagnosis of a congenital developmental defect in a child poses the following questions to the neonatologist:
What type of pathology does this defect belong to (congenital malformation, disruption, deformation or dysplasia)?
How often is this birth defect associated with other birth defects or diseases that are not yet clinically apparent?
How often is this birth defect a symptom of the syndromic form of the pathology?
What syndromes are most common with this birth defect?
The answers to these questions are the first diagnostic stage practical collaboration neonatologist and geneticist. Final goal This stage includes the diagnosis of additional congenital developmental defects or the diagnosis of a specific syndrome. In the case of diagnosing a syndromic form of pathology, in most cases, further medical tactics regarding conservative or surgical treatment and medical and genetic prognosis in the family of a sick child. Information about the prognosis for life and health with a particular syndrome has great importance and is the main goal of medical work.
Syndromes can be analyzed at different levels of biological organization:
At the level of disorders within metabolic processes (dysmetabolic syndromes);
At the level of tissue disorders (dysplasia syndromes);
At the level of organ morphology disorders (congenital malformation syndromes and disruption syndromes);
At the level of disorders of a certain area of the body (deformation syndromes). All four levels of violations have and practical significance, since all four biological types of syndromes have clear diagnostic and genetic criteria for diagnosis and prognosis for health (Table 36-12).
Diagnosis of syndromic forms of pathology in a newborn includes:
Opportunity accurate diagnosis concomitant diseases a child with multiple defects;
Forecast of complications characteristic of each syndrome during surgical or conservative treatment birth defects or diseases;
Accurate assessment of the possibilities of surgical or conservative treatment of diseases (timing and volume of surgical intervention, long-term results treatment);
Accurate medical and genetic prognosis in the family.
These conclusions are well illustrated by the following observations from clinical practice.
Table 36-12. Biological types syndromes (Cohen M.M., 1982)
| Type of syndrome (level of impairment) | Characteristic signs | Examples |
| Dysmetabolic syndrome (metabolism) Dysplasia syndrome (tissue) | Newborns have a normal phenotype with a progradient clinical picture. Clinical signs relatively similar compared to other types of syndromes. There is no association with congenital malformations. Verification of the primary biochemical defect is possible. Autosomal recessive type of inheritance Simple dysplasia syndrome is characterized by damage only | PKU, Tay-Sachs disease, VGS Marfan syndrome, Ehlers-Danlos syndrome, achondroplasia |
| one germ layer. | ||
| Dominant or recessive type | ||
| inheritance | ||
| Hamartoneoplastic | Neurofibromatosis | |
| syndrome: | Two or three germinal cells are involved | Recklinghausen |
| leaf; | ||
| tendency to neoplasia; | ||
| usually dominant mode of inheritance | ||
| Developmental defect syndrome or | Down syndrome, | |
| corruption (organs) | Two or more developmental defects in one | TAR syndrome, |
| newborn Characterized by | alcoholic syndrome | |
| embryonic pleiotropy. | fetus | |
| Biochemical verification | ||
| impossible or rare. Etiology | ||
| different - monogenic, chromosomal | ||
| or teratogenic | ||
| Deformity syndrome (area | ||
| body) | Violation of form or position | Potter syndrome |
| initially normally formed | ||
| organs or body parts. | ||
| Most cases are explained | ||
| violation motor activity | ||
| fetus (hypokinesia). | ||
| The musculoskeletal system is usually affected | ||
| system. |
A birth defect is an abnormality in the body structure or chemistry of a newborn baby. This may be caused hereditary factors (genetic reasons), as a result of exposure environment, which affects the embryo or fetus in the womb, or a combination of factors. Often the causes of birth defects cannot be determined.
Birth defects are sometimes called congenital anomalies. Abnormalities that are present at birth are generally not considered a birth defect unless they result in illness or physical or mental disability. For example, moles are rarely considered a birth defect because they usually do not cause health problems.
It is estimated that 3 to 5 percent of children have some type of birth defect. Some birth defects occur infrequently. Others, such as some congenital heart defects, are more common.
Hereditary factors and birth defects
Each of us has genes inherited from our parents. Genes determine our innate characteristics or traits. In the case of birth defects, genes can also influence the abnormalities.
A child inherits two copies of each gene, one from the mother and one from the father. If the defective gene is dominant, the child who inherits that copy will have the defect. This occurs because the defective copy "dominates" the normal copy inherited from the other parent. But if the defective gene is recessive, the child will inherit two defective copies: one from the mother and one from the father.
Examples of autosomal dominant birth defects include Huntington's disease, a nervous system disorder, and Marfan syndrome, which is characterized by long bones and heart problems. Some congenital diseases, such as Huntington's disease, have no symptoms for many years.
Other birth defects are determined by genes on the X chromosome (the X and Y chromosomes determine the sex of the baby). Hemophilia, congenital blood disorders, and color blindness are examples of X-chromosomal birth defects.
Many inherited birth defects, however, are not simply dominant, recessive or X-chromosomal; there are also multiple defective genes.
Chromosomal abnormalities
Some birth defects are caused by extra, missing, incomplete, or misshapen chromosomes. Down syndrome, one of the most common birth defects, is usually caused by the presence of an extra chromosome in cells. Down syndrome is characterized by mental retardation, short stature and distinctive features faces. Defects associated with sex chromosomes can lead to problems with sexual development, including sterility (the inability to have children).
Environmental factors
Birth defects can also be caused by environmental factors. The environment here means the mother's body, however, scientists are studying possible impact on the occurrence of birth defects and environmental conditions of the Earth.
 Pregnant women who consume excessive amounts of early stages have pregnancy increased risk give birth to children with fetal alcohol syndrome. Children with this congenital disease may have various defects in growth, appearance and mental abilities. And even moderate alcohol consumption can cause fetal harm. Smoking during pregnancy increases the likelihood that the baby will have a lower birth weight and increases the risk of other birth defects.
Pregnant women who consume excessive amounts of early stages have pregnancy increased risk give birth to children with fetal alcohol syndrome. Children with this congenital disease may have various defects in growth, appearance and mental abilities. And even moderate alcohol consumption can cause fetal harm. Smoking during pregnancy increases the likelihood that the baby will have a lower birth weight and increases the risk of other birth defects.
Some diseases in pregnant women, for example, can lead to deafness, blindness and congenital heart defects in the child. Venereal diseases can be transmitted to the fetus or newborn.
Some medications have been linked to birth defects. The best known is thalidomide. sedative. Many other medications, including tranquilizers, antibacterials and antitumor drugs, can cause congenital abnormalities.
Other environmental factors which are believed to increase the risk of birth defects include poor nutrition and mother's age. For example, the older a pregnant woman is, the more likely she is to give birth to a child with Down syndrome.
Diagnosis of birth defects
 Some birth defects can be diagnosed while the baby is still in the womb. A procedure that uses ultrasonic waves to obtain an image of the fetus on a screen, can help the doctor detect some malformations. For example, some spinal defects can be detected using ultrasound.
Some birth defects can be diagnosed while the baby is still in the womb. A procedure that uses ultrasonic waves to obtain an image of the fetus on a screen, can help the doctor detect some malformations. For example, some spinal defects can be detected using ultrasound.
In a procedure called , a small sample of the fluid surrounding the fetus is examined. This test is useful for detecting congenital metabolic defects and chromosomal abnormalities.
Many birth defects can be diagnosed through a physical examination of the newborn baby by a doctor. Other tests including X-rays, may be used if doctors suspect birth defects. Blood tests can detect certain abnormalities in blood or body chemistry.
Treatment of birth defects
Not every birth defect affects the quality of life of the person who has it. Some birth defects have little effect, except perhaps in appearance.
Some birth defects can be treated to prevent or reduce them harmful effects. Surgery can perform operations to correct congenital malformations such as clubfoot, cleft palate, cleft lip, structural and gastrointestinal tract. Treatment may reduce symptoms of cystic fibrosis, hereditary disease associated with breathing. In some cases, disorders such as hydrocephalus can be corrected before birth.
 Doctors can sometimes treat congenital disorders body chemistry through drugs and special diets. For example, fast treatment may prevent brain damage from phenylketonuria, a metabolic defect that can lead to severe mental retardation. Special education, rehabilitation, as well as the use of special devices and devices can help compensate for some mental and physical disabilities, such as blindness and deafness.
Doctors can sometimes treat congenital disorders body chemistry through drugs and special diets. For example, fast treatment may prevent brain damage from phenylketonuria, a metabolic defect that can lead to severe mental retardation. Special education, rehabilitation, as well as the use of special devices and devices can help compensate for some mental and physical disabilities, such as blindness and deafness.
Prevention of birth defects
No one can guarantee that a child will be born “perfect” and healthy. However, there are ways to minimize your baby's chances of having birth defects.
Pregnant women should not smoke or use alcoholic drinks, they should not consume medications of any kind unless prescribed by a doctor. Some vitamins, if taken in proper amounts, can help prevent some birth defects. For example, folic acid during pregnancy may help prevent some spinal and central nervous system defects. Vaccinations well before pregnancy can prevent birth defects that can occur as a result of illnesses during pregnancy.
Denial of responsibility: The information presented in this article about birth defects is for the reader's information only. It is not intended to be a substitute for advice from a healthcare professional.
