Restoration of fat metabolism. Fat metabolism disorder, treatment, symptoms, folk remedies
Lipid metabolism disorders can occur as a result of disturbances: 1) absorption of fat in the intestine; 2) transfer of fat from blood to tissue; 3) fat deposition: 4) interstitial fat metabolism.
§ 198. Malabsorption of fat
For the absorption of dietary fat from the intestine, it must be emulsified, broken down into glycerol and fatty acid and the formation of complex compounds with bile acids - choleinates. Therefore, the cessation of bile secretion in duodenum or a decrease in its secretion immediately affects the digestion of fats. Blockage of the bile duct, inflammation of the gallbladder (cholecystitis) and some liver diseases associated with disruption of the process of bile secretion lead to the fact that non-emulsified fats pass through the digestive canal, being exposed only in limited quantities. to a large extent hydrolysis. If the hydrolysis of dietary fats is carried out sufficiently under the action of lipases of pancreatic and intestinal juices, then the resulting fatty acids are still not absorbed. The same thing happens with a decrease or complete cessation of the secretion of pancreatic enzymes, with a decrease in the function of the intestinal epithelium and with significantly increased peristalsis small intestine when fat does not have time to be absorbed. This kind of fat absorption disorder is observed in enteritis, hypovitaminosis A and B, due to a disruption in the formation of enzymes involved in the resynthesis of triglycerides in the intestinal epithelium.
The secretion of fat occurs mainly through the intestines and to a lesser extent is carried out by sebaceous and sweat glands. Only traces of fat are found in the urine. If there is a malabsorption of fat, the feces contain a lot of undigested fat and higher fatty acids and have a characteristic grayish-white color - steatorrhea. Excretion of fat in the urine - lipuria - can occur after ingesting very large amounts of fat with food, with fractures of long bones accompanied by crushing bone marrow, trauma to large areas of adipose tissue, with lipoid nephrosis.
Excessive fat production sebaceous glands- seborrhea - occurs in some skin diseases - acne, eczema, vitamin deficiencies, etc.
Consequences of malabsorption of fat- although fats and lipids are easily synthesized in the body from intermediate products of carbohydrate metabolism, complete exclusion of fats from food is unacceptable. Vital fat-soluble vitamins (A, D, E, K) are introduced into the body with fats, and therefore, with insufficient intake of fats from food, hypovitaminosis can develop in humans and animals. In addition, natural fats always contain small amounts of essential unsaturated fatty acids (for example, linoleic-C 18 H 32 O 2 and linolenic - C 18 H 30 O 2), which cannot be synthesized in the body from other fatty acids. In the absence of them in food, experimental animals develop chronic diseases skin (in the form of necrotic foci). Apparently complete absence unsaturated higher fatty acids in human food may also cause more or less serious disorders exchange.
§ 199. Violation of the transition of fat from blood to tissue
Neutral fat coming from the intestines circulates in the blood in the form of chylomicrons (consisting of triglycerides, cholesteryl esters, phospholipids and β-lipoprotein) and α-lipoproteins. The normal content of neutral fats in the blood is 1-2 g/l.
A temporary transient increase in the content of chylomicrons in the blood - hyperlipemia - is observed with an increased intake of fat from food ( nutritional hyperlipemia). Hyperlipemia may result from increased mobilization of fat from the depot - transport hyperlipemia(Fig. 35).
Many hormones contribute to the mobilization of fat from fat depots, lungs, and bone marrow. For example, during fasting, the release of fat from its depot occurs as a result of the combined action of pituitary growth hormone, pancreatic glucagon and adrenaline. The effect of these hormones on adipose tissue is realized through the adenyl cyclase system - tAMP. The latter increases the activity of triglyceride lipase, which carries out lipolysis in tissues.
Mobilization of fat from the lungs, leading to hyperlipemia, occurs mainly with prolonged hyperventilation of the lungs, for example in professional singers.
Retention hyperlipemia(retentio - delay) - the result of a delay in the transition of neutral fats from the blood to the tissues, occurs mainly when the content of albumin and clearing factor (FP), a specific lipoprotein lipase, decreases in the blood. Under the influence of AF, the breakdown of triglycerides associated with proteins occurs and thereby “clarification” of the lipemic serum. The resulting free fatty acids are bound by albumin (1 molecule of albumin binds 6-7 molecules of fatty acids), which promotes the transfer of fat into cells. Therefore, a lack of albumin in the blood (for example, during fasting, kidney disease - nephrosis) leads to hyperlipemia, as well as insufficient levels of AF and heparin. For example, in atherosclerosis, hyperlipemia depends on a decrease in heparin content and low lipoprotein lipase (LP) activity. In diabetes, a decrease in FP in the blood depends on the lack of lipocaine.
§ 200. Excessive accumulation of fat in adipose tissue
Obesity is the result of dysregulation of fat entry into adipose tissue, its formation and utilization as a source of energy.
One of the significant causes of obesity is excessive (relative to energy expenditure) food consumption associated with increased appetite. The latter is due to increased excitability of the food center, in particular nerve formations hypothalamic region. It has been experimentally established that irritation of the ventrolateral nuclei of the hypothalamus and destruction of the ventromedial ones cause a lack of satiety, increased appetite, hyperphagia with subsequent fat deposition (the so-called hypothalamic obesity).
The clinical analogue of this type of obesity is diencephalic obesity, which develops as a result of infectious and toxic damage to nerve formations in the interstitial brain, as well as tumors in this area.
A decrease in the release of fat from its depot occurs when the function is suppressed thyroid gland and the pituitary gland, whose hormones (thyroxine, growth hormone, TSH) activate the mobilization of fat and its subsequent oxidation. Increased production of pituitary ACTH, adrenal glucocorticoids and insulin promotes fat deposition and its formation from carbohydrates. Decreased function of the gonads leads to excess fat deposition if it is accompanied by disruption of the activity of the hypothalamic centers (see §§ 337, 338).
§ 201. Fatty infiltration of the liver
If the fat transported by blood to the cells does not undergo breakdown and oxidation in them, it is not excreted long time remains in cells, arises fatty infiltration(impregnation). Its combination with a violation of the protoplasmic structure is called fatty degeneration.
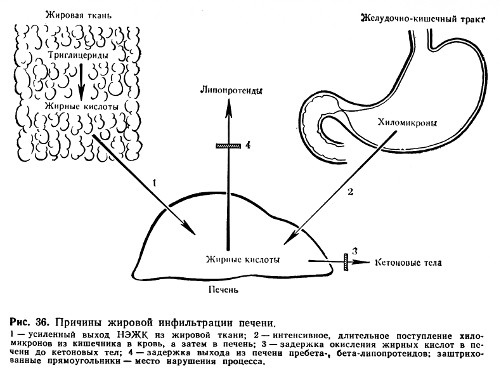
The common cause of fatty infiltration and degeneration is the suppression of the activity of hydrolytic and oxidative enzymes of fat metabolism (Fig. 36), which can be observed in case of poisoning with phosphorus, arsenic, chloroform, viral infections, avitaminosis (alcoholism).
Great importance in the pathogenesis of fatty liver infiltration is attributed to a violation of the formation of phospholipids. Their sufficient content in the liver ensures fine dispersion of fat and thereby its exit from the cell. The phospholipid molecule catalyzes the oxidation of fatty acids. Insufficient formation of phospholipids occurs when there is a deficiency in the body of choline, a structural part of the main phospholipid of the liver - lecithin. And the synthesis of choline, in turn, is associated with methyl groups, the donor of which is the amino acid methionine. Therefore, insufficient introduction of dietary choline into the body or insufficient formation of it due to lack of methionine can lead to fatty infiltration of the liver. Methionine, like the protein casein, which contains a large number of methionine, has a lipotropic effect, that is, it helps remove excess fat from the liver. The same property is possessed by the endogenous lipotropic factor - lipocaine (formed in the epithelium of the small ducts of the pancreas). Lack of lipocaine in diabetes mellitus promotes fatty infiltration of the liver.
§ 202. Disorders of intermediate fat metabolism
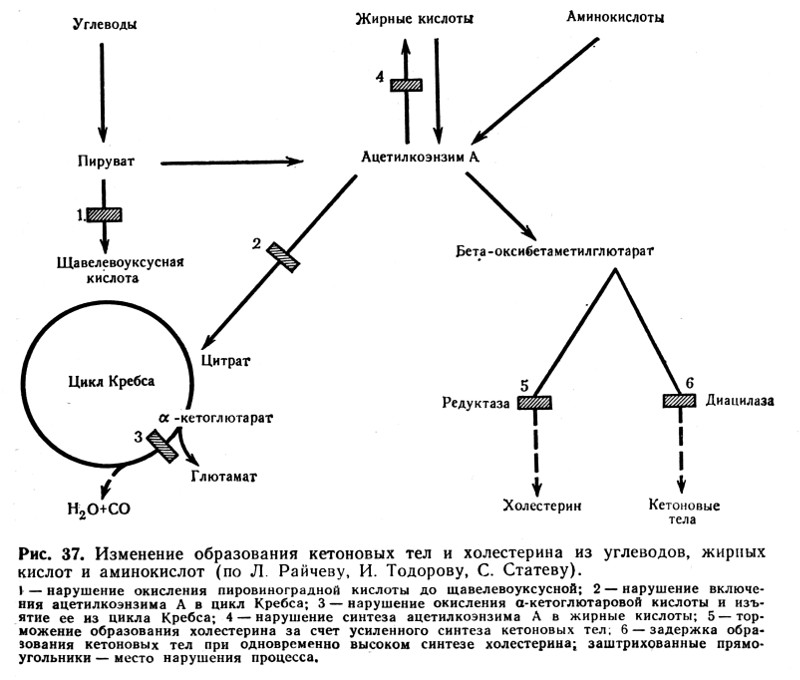
Relatively stable products of interstitial metabolism of higher fatty acids are acetone, acetoacetic and beta-hydroxybutyric acids, the so-called ketone or acetone bodies, formed mainly in the liver and oxidized to CO 2 and H 2 O in other tissues and organs (muscles, lungs, kidneys and etc.). In some pathological processes and diseases (diabetes mellitus, fasting - complete or exclusively carbohydrate, long-term infections with high temperature, hypoxia, diseases of the liver parenchyma, etc.), the content of acetone bodies in the blood can increase sharply (normally their content does not exceed 0.02-0.04 g/l) (2-4 mg%). Acetonemia leads to the appearance of ketone and acetone bodies in the urine - aceturia. Acetone is excreted not only through the kidneys, but also through the lungs with exhaled gases and sweat. The patient smells of acetone.
Mechanisms leading to an increase ketone bodies in the blood (ketosis) are quite complex.
- One of the main reasons for the development of ketosis is a deficiency of carbohydrates (for example, in diabetes mellitus, fasting), which leads to depletion of the liver in glycogen and increased entry of fat into it, where the oxidation of fatty acids to acetoacetic acid occurs. This is also facilitated by insufficient resynthesis of higher fatty acids from ketone bodies and a violation of their oxidation in the tricarboxylic (citric) cycle. Resynthesis requires energy from glycolysis. Insufficient oxidation of ketone bodies is also associated with a deficiency of compounds formed during intermediate carbohydrate metabolism (pyruvic and oxaloacetic acids) and which are substrates of the tricarboxylic acid cycle (Fig. 37).
- An important pathogenetic link in the development of ketosis in diabetes mellitus is the simultaneous deficiency of lipocaine and insulin.
- With liver damage caused by toxin-infectious factors, the glycogen-forming function of the liver is impaired, which promotes the transfer of fatty acids to the liver. Here, the formation of ketone bodies largely prevails over their oxidation. The result is ketosis and fatty liver.
§ 203. Disorders of phospholipid metabolism
Disorders of phospholipid metabolism (lecithins, cephalins) are closely related to fat metabolism. Thus, with lipemia, the level of lecithin in the blood increases.
There are some hereditarily determined pathological conditions associated with excessive deposition of phospholipids in tissues. For example, in Gaucher disease, cerebrosides are deposited in macrophage cells of the spleen, liver, lymph nodes and bone marrow. In Niemann-Pick disease in cells various organs deposition of sphingomyelin phosphatide is observed. Amaurotic (from the Greek amauros - dark, blind) familial idiocy is the result of the deposition of lipoids in nerve cells, which is accompanied by optic nerve atrophy and dementia.
§ 204. Cholesterol metabolism disorders. Atherosclerosis
Cholesterol metabolism disorders underlie the development of atherosclerosis, cholelithiasis, lipoid nephrosis, age-related opacification of the cornea, xanthomatosis of the skin, bones and other diseases.
Russian pathophysiologists N.P. Anichkov and S.S. Khalatov played a major role in the study of cholesterol metabolism disorders. Back in 1911-1912. They created an experimental model of atherosclerosis by feeding cholesterol to animals. Although in the pathogenesis of human atherosclerosis the importance of exogenous cholesterol (from food) is not so significant, the fact of a disorder in cholesterol metabolism is beyond doubt.
Under physiological conditions, the cholesterol content in the blood of an adult is about 1.8-2.3 g/l. Some increase in blood cholesterol levels may occur after eating cholesterol-rich foods ( egg yolk, brain, liver, butter etc.), but this nutritional hypercholesterolemia in humans is rapidly passing, because with an excess of cholesterol from mast cells Heparin is released into the blood, activating lipoprotein lipase, the so-called “clearing factor” (FP). The latter converts large-molecular lipids with low density into finely dispersed ones that are easily removed from the blood.
Changes in cholesterol metabolism may be the result of impaired cholesterol synthesis, leading to endogenous hypercholesterolemia. Cholesterol synthesis is regulated primarily by its intake from the intestines: a small intake activates cholesterol synthesis. The starting material for the synthesis of cholesterol is, in addition to acetoacetic acid, the amino acids valine and leucine, fatty acids, carbohydrates, which in the process of interstitial metabolism are converted into acetyl coenzyme A. The latter is included in the beta-hydroxy-beta-methyl-glutaryl coenzyme A cycle and contributes to the development of hypercholesterolemia.
An important factor in cholesterol metabolism is the activity of tissue enzymes that ensure the breakdown of lipids. Thus, it has been proven that when pathological conditions, predisposing to atherosclerosis (diabetes, stress, hypoxia), the lipolytic activity of the aortic wall is significantly reduced, and the cholesterol content in it increases sharply. The aortic wall of healthy people contains 5-50 mg of cholesterol, in the atheromatous aorta - 240 mg, with severe forms atheromatosis, the cholesterol content in the aorta can reach 500-1000 mg.
The cause of hypercholesterolemia may also be a change in the physicochemical state of blood proteins, due to which a stronger bond between cholesterol and β-lipoproteins is formed and the release of cholesterol from the complex is difficult, or, conversely, the β-protein complex is broken and the dispersion of cholesterol micelles decreases. In both cases, cholesterol is retained in the blood.
In violation of cholesterol metabolism, loss of function of the thyroid, gonads, and adrenal glands is important. Which parts of cholesterol metabolism are changed by each of these hormones is a very complex question. They can change the rate of cholesterol transfer into and out of the cell, influence the distribution of its fractions between blood plasma and interstitial fluid, and the processes of cholesterol synthesis and breakdown.
The most important manifestation of cholesterol metabolism disorders in the human body is atherosclerosis.
Lipids- heterogeneous in chemical composition organic matter, insoluble in water, but soluble in non-polar solvents.
Typical forms of lipid metabolism pathology are obesity, exhaustion, lipodystrophy, lipidosis and dyslipoproteinemia.
Obesity
Obesity- excess accumulation lipids in the body in the form of triglycerides.
TYPES OF OBESITY
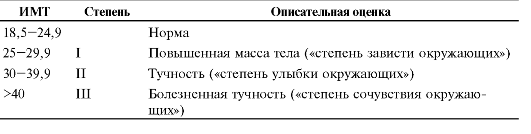
Depending on the degree of weight gain There are three degrees of obesity.
Various formulas are used to estimate optimal body weight.
♦ The simplest is the Broca index: 100 is subtracted from the height indicator (in cm).
♦ Body mass index (BMI) is also calculated using the following formula:
Depending on the value of the body mass index, they speak of normal or overweight of 3 degrees (Table 10-1).
According to the predominant localization of adipose tissue distinguish between general (uniform) and local obesity (local lipohypertrophy). There are two types of local obesity.
♦ Female type(gynoid) - excess subcutaneous fat mainly in the hips and buttocks.
Table 10-1. Obesity levels
 ♦ Male type(android or abdominal) - accumulation of fat mainly in the abdominal area.
♦ Male type(android or abdominal) - accumulation of fat mainly in the abdominal area.
By genesis There are primary obesity and its secondary forms.
♦ Primary (hypothalamic) obesity is an independent disease of neuroendocrine origin, caused by a disorder of the fat metabolism regulation system.
♦ Secondary (symptomatic) obesity is a consequence various violations in the body, causing a decrease in lipolysis and activation of lipogenesis (for example, in diabetes, hypothyroidism, hypercortisolism).
ETIOLOGY
The cause of primary obesity is a dysfunction of the hypothalamus-adipocyte system.
Secondary obesity develops due to excess calorie intake and reduced level energy consumption of the body (mainly during physical inactivity).
PATHOGENESIS OF OBESITY
There are neurogenic, endocrine and metabolic mechanisms of obesity.
Neurogenic variants of obesity
Centrogenic(cortical, psychogenic) mechanism - one of the variants of eating disorder (the other two: anorexia nervosa and bulimia).
♦ Cause: various mental disorders, manifested by a constant, sometimes irresistible desire to eat.
♦ Possible mechanisms:
❖ activation of serotonergic, opioidergic and other systems involved in the formation of feelings of pleasure and comfort;
❖ perception of food as a strong positive stimulus (doping), which further activates these systems. This
closes the vicious circle of the centrogenic mechanism of obesity development.
Hypothalamic(diencephalic, subcortical) mechanism.
♦ Cause: damage to hypothalamic neurons (for example, after a concussion, encephalitis, craniopharyngioma, metastases of tumors to the hypothalamus).
♦ The most important links in pathogenesis:
❖ Damage or irritation of neurons in the posterolateral ventral nucleus of the hypothalamus stimulates the synthesis and secretion of neuropeptide Y and reduces sensitivity to leptin, which inhibits the synthesis of neuropeptide Y. Neuropeptide Y stimulates hunger and increases appetite.
❖ Impaired formation of the feeling of hunger due to excessive production of neurotransmitters that form the feeling of hunger and increase appetite (GABA, dopamine, β-endorphin, enkephalins). This leads to a decrease in the synthesis of neurotransmitters that create a feeling of satiety and inhibit eating behavior (serotonin, norepinephrine, cholecystokinin, somatostatin).
Endocrine variants of obesity
The endocrine mechanisms of obesity are leptin, hypothyroid, adrenal and insulin.
Leptin mechanism- leading in the development of primary obesity.
♦ Leptin formed in fat cells. It reduces appetite and increases energy expenditure by the body. Leptin suppresses the formation and release of neuropeptide Y by the hypothalamus.
♦ Neuropeptide Y participates in the formation of hunger. It increases appetite and reduces the body's energy expenditure.
♦ Lipostat. The leptin-neuropeptide Y circuit ensures the maintenance of body fat mass with the participation of insulin, catecholamines, serotonin, cholecystokinin, and endorphins. In general, this system of biologically active substances, which ensure dynamic homeostasis of energy metabolism and adipose tissue mass in the body, is called the lipostat system.
Hypothyroid mechanism obesity is activated when the effects of iodine-containing thyroid hormones are insufficient, which reduces the intensity of lipolysis, the rate of metabolic processes in tissues and the body’s energy costs.
Adrenal(glucocorticoid, cortisol) mechanism obesity is activated due to hyperproduction of glucocorticoids in the adrenal cortex (for example, in disease and syndrome
Itsenko-Cushing), which promotes lipogenesis due to hyperglycemia and activation of the insulin mechanism.
Insulin mechanism The development of obesity develops as a result of direct activation of lipogenesis in adipose tissue by insulin.
Metabolic mechanisms of obesity. The reserves of carbohydrates in the body are relatively small. In this regard, a mechanism for saving carbohydrates has been developed: with an increase in the proportion of fat in the diet, the rate of carbohydrate oxidation decreases. When the regulatory system is disrupted, a mechanism is activated that increases appetite and food intake. Under these conditions, fats are not broken down and accumulate in the form of triglycerides.
Exhaustion
Exhaustion- pathological decline fat mass, as well as muscle and connective tissue below normal. Extreme degree exhaustion is cachexia.
With exhaustion, the deficit of adipose tissue is more than 20-25%, and with cachexia - more than 50%. BMI for exhaustion is less than 19.5 kg/m2.
ETIOLOGY
Depletion can be caused by endogenous and exogenous reasons.
Exogenous causes:
♦ Forced or conscious complete or partial fasting.
♦ Insufficient caloric content of food.
Endogenous causes of exhaustion are divided into primary and secondary.
♦ Cause of primary exhaustion: suppression of the synthesis of neuropeptide Y in the hypothalamus (with trauma or ischemia of the hypothalamus, severe prolonged stress) and hyposensitization of target cells to neuropeptide Y.
♦ Causes of secondary (symptomatic) exhaustion: malabsorption, glucocorticoid deficiency, hypoinsulinism, increased synthesis of glucagon and somatostatin, overproduction of TNFα by tumor cells.
PATHOGENESIS
Exogenous wasting and cachexia. The absence or significant deficiency of food leads to depletion of fat reserves, disruption of all types of metabolism, insufficiency of biological oxidation and suppression of plastic processes.
Primary endogenous forms of wasting
Greatest clinical significance have hypothalamic, cachectic and anorexic forms.
In the hypothalamic (diencephalic, subcortical) form of exhaustion and cachexia, there is a decrease or cessation of synthesis and release of peptide Y into the blood by hypothalamic neurons, which disrupts lipostat.
In the cachectin (or cytokine) form of depletion, the synthesis of TNFa (cachectin) by adipocytes and macrophages leads to suppression of the synthesis of neuropeptide Y in the hypothalamus, inhibition of lipogenesis and activation of lipid catabolism.
Anorexic form.
♦ In people with a predisposition to anorexia, a critical attitude towards their body weight (perceived as excessive) leads to the development of neuropsychiatric disorders and long periods refusal to eat. It is most often observed in teenage girls and girls under 18 years of age.
♦ The further course of the process is associated with a decrease in the synthesis of neuropeptide Y and a significant decrease in body weight, up to cachexia.
Secondary endogenous forms exhaustion and cachexia are symptoms of other forms of pathology: malabsorption syndromes, growth of neoplasms (synthesizing TNF), hypoinsulinism, hypocortisolism, lack of effects of thymus hormones.
Lipodystrophies and lipidoses
Lipodystrophy- conditions characterized by generalized or local loss of adipose tissue, less often - its excessive accumulation in the subcutaneous tissue.
Lipidoses- conditions characterized by disorders of lipid metabolism in cells (parenchymal lipidoses), fatty tissue (obesity, wasting) or walls arterial vessels(for example, with atherosclerosis).
Dyslipoproteinemia
Dyslipoproteinemia- conditions characterized by deviations from the norm in the content, structure and ratio of various drugs in the blood.
The nature of the current and clinical manifestations dislipoproteinemia is determined by:
♦ genetic characteristics organism (for example, composition, ratio and level of various drugs);
♦ factors external environment(for example, a set of food products, dietary features and eating patterns);
♦ availability concomitant diseases(for example, obesity, hypothyroidism, diabetes, kidney and liver damage).
Atherogenicity of lipoproteins
LPs are divided into atherogenic (VLDL, LDL and LPPP) and antiatherogenic (HDL).
The potential atherogenicity of blood lipids is assessed by calculating the cholesterol atherogenicity coefficient:
total cholesterol - HDL cholesterol
HDL cholesterol
Normally, the cholesterol atherogenic coefficient does not exceed 3.0. As this value increases, the risk of developing atherosclerosis increases.
TYPES OF DYSLIPOPROTEINEMIA
By origin: primary (hereditary; they can be monogenic and polygenic) and secondary.
According to changes in the content of lipoproteins in the blood: hyperlipoproteinemia, hypo- and alipoproteinemia, combined dislipoproteinemia.
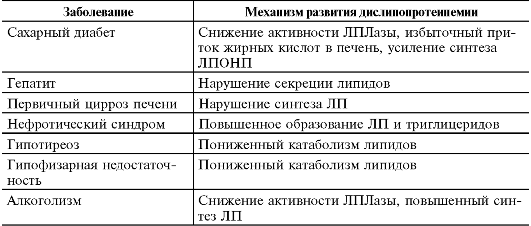
Various, usually chronic, diseases can lead to the development of secondary dislipoproteinemia (Table 10-2).
Table 10-2. Diseases leading to the development of secondary dislipoproteinemia
 Hyperlipoproteinemia
Hyperlipoproteinemia
Hyperlipoproteinemia- conditions manifested by a persistent increase in the content of drugs in the blood plasma.
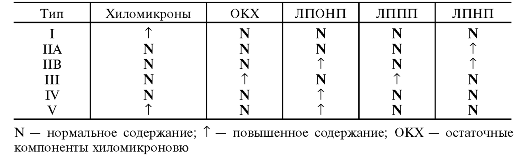
In 1967, Fredrickson et al. developed a classification of hyperlipoproteinemia. This classification was later revised by WHO specialists (Table 10-3).
Table 10-3. Types of hyperlipoproteinemia and the content of various lipoproteins with them
 Hypolipoproteinemia
Hypolipoproteinemia
Hypolipoproteinemia- conditions manifested by a persistent decrease in the level of drugs in the blood plasma up to their complete absence (alipoproteinemia).
Combined dyslipoproteinemia are characterized by a violation of the ratio of various drug fractions.
Atherosclerosis
Atherosclerosis- a chronic pathological process leading to changes mainly in the inner lining of arteries of the elastic and muscular-elastic types due to the accumulation of excess lipids, the formation fibrous tissue, as well as a set of other changes in them.
In atherosclerosis, the most commonly affected arteries are the coronary, carotid, renal, mesenteric, lower limbs, as well as the abdominal aorta.
ETIOLOGY
Causes atherosclerosis has not been fully elucidated. There are three hypotheses explaining the occurrence of atherosclerosis: lipid, chronic endothelial damage and monoclonal.
Risk factors. At least 250 factors are known that contribute to the emergence and development of atherosclerosis. The most significant risk factors include smoking, diabetes, arterial hypertension, obesity, autoimmune diseases, hypercholesterolemia, hypertriglyceridemia, hyperhomocysteinemia, physical inactivity, hereditary predisposition, taking oral contraceptives.
PATHOGENESIS
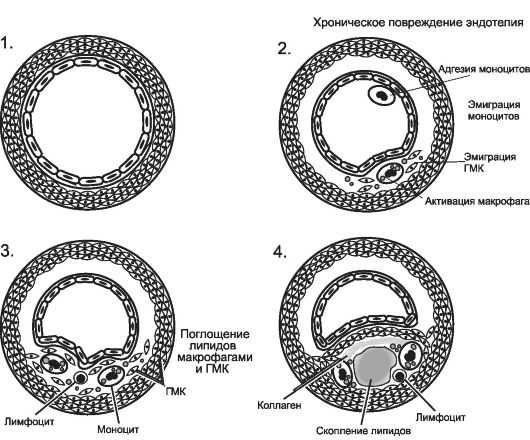
Highlight next stages atherosclerotic vascular damage: lipid spots and stripes, formation of atheroma and fibroatheroma, development of complications (Fig. 10-1).
Lipid spots and streaks
Intact endothelium prevents the penetration of drugs into the intima of the arteries. Under the influence of risk factors, endothelial cells are damaged and develop endothelial dysfunction- trigger factor atherogenesis.
The formation of lipid spots and streaks occurs in several stages:
♦ Migrations to the intimal areas of arteries with damaged endothelial cells large number monocytes and T-lymphocytes.
♦ Synthesis of biologically active substances (chemotaxis factors, kinins, Pg, TNFa) and reactive oxygen species by leukocytes, which is accompanied by intensification of lipid peroxidation. These factors potentiate endothelial damage and penetration of drugs into the vascular intima.
♦ Additional activation of peroxidation of LDL penetrating into the subendothelial layer with the formation of modified LP.
♦ Capture of modified drugs by monocytes using “scavenger receptors” (scavenger receptors) and converting them into foam cells- lipid-rich macrophages.
♦ Activation of T-lymphocytes and macrophages at the site of damage to the artery wall with the development of aseptic inflammation.
♦ Proliferation of SMCs and fibroblasts and their synthesis of connective tissue components with the formation of lipid spots and stripes in the intima.
Formation of atheroma and fibroatheroma
The formation of an atherosclerotic plaque is caused by several factors:
Further damage to the endothelium mediators of inflammation, which potentiates the penetration of LDL into the vascular intima and the closure of a vicious circle.
 Rice. 10-1.
Consecutive changes in the damaged arterial wall in atherosclerosis. 1 - normal artery wall; 2 - adhesion of monocytes and platelets to damaged endothelium; 3 - migration of monocytes and SMCs into the intima, lipid infiltration; 4 - proliferation of cellular elements, formation of a lipid core and formation of fibroatheroma. [by 4].
Rice. 10-1.
Consecutive changes in the damaged arterial wall in atherosclerosis. 1 - normal artery wall; 2 - adhesion of monocytes and platelets to damaged endothelium; 3 - migration of monocytes and SMCs into the intima, lipid infiltration; 4 - proliferation of cellular elements, formation of a lipid core and formation of fibroatheroma. [by 4].
Transformation SMCs into macrophage-like and activation of the synthesis by them and fibroblasts of the components of the intercellular substance of connective tissue (proteoglycans, glycosaminoglycans, collagen and elastic fibers).
Formation of the lipid core atheroma due to the death of foam cells and the release of free lipids from them.
♦ Atheroma characterized by the presence of a significant number of cellular elements: foam cells, SMCs on different stages proliferation and transformation, lymphocytes, granulocytes, platelets; the formation of a lipid core with a large amount of free cholesterol and its esters.
♦ Fibroatheroma characterized by the formation of a fibrous cap over the lipid core due to the synthesis of connective tissue components and the development of a network of newly formed vessels penetrating the plaque.
Development of complications of atherosclerosis
Modification atherosclerotic plaques leads to the development of the following processes:
♦ calcifications, atherocalcinosis - accumulation of calcium compounds in plaque tissue;
♦ cracks in the fibroatheroma cover or its ulcerations, which is accompanied by the development of a parietal thrombus with the threat of artery obstruction or embolism;
♦ ruptures of the walls of newly formed microvessels, leading to hemorrhages into the arterial wall, the formation of parietal and intramural thrombi.
Clinically, complications of atherosclerosis most often manifest themselves as ischemia and infarction of organs and tissues supplied with blood from the affected artery.
PRINCIPLES OF PREVENTION AND THERAPY OF ATHEROSCLEROSIS
Etiotropic. The goal is to eliminate or reduce the effect of risk factors. Examples of measures: use of lipid-lowering drugs, correction of blood pressure, smoking cessation, adherence to a certain diet.
Pathogenetic. Aimed at breaking the “chain of atherogenesis”. Examples of impacts: use of antiplatelet agents and anticoagulants; the use of specific drugs that reduce inflammation in atheroma (for example, statins or monoclonal antibodies to TNF and other proinflammatory cytokines).
The term “metabolism” means everything chemical reactions that occur in the body. Life without them human body becomes impossible, because only thanks to such processes do cells exist: grow, contact with the outside world, feed and cleanse themselves. There are quite a few types of metabolism; proteins, fats, and amino acids take part in them. And in some cases, the course of such processes may be disrupted, which requires appropriate correction. Let's talk on the www.site about what a fat metabolism disorder is, consider its treatment and symptoms, as well as folk remedies which will help to cope with this problem.
The term “fat metabolism” refers to the production and breakdown of fats (lipids) within the body. The processes of fat breakdown are carried out mostly in the liver, as well as in adipose tissue. And failures in normal metabolism lipids can cause the development of atherosclerosis, obesity, as well as various endocrine diseases (for example, diabetes). As is known, fat metabolism is characterized by particularly complex regulation. It is influenced by insulin, sex hormones, as well as adrenaline, thyroxine and other hormones.
About how lipid metabolism disorder manifests itself, what symptoms indicate the disease
Fat metabolism occurs in almost all cells and tissues of the body. It is for this reason that the symptoms of its disorders are difficult to localize, and they are difficult to divide into primary or secondary.
The most basic and noticeable sign of the disorder is a noticeable increase in the volume of subcutaneous fat, which is the main fat depot in the body. In the event that the process of such accumulation occurs with particular intensity, doctors raise the issue of obesity and consider it as an independent disease. Obesity itself makes itself felt nearby unpleasant symptoms. Such a violation causes a decrease physical capabilities, provokes shortness of breath, snoring, etc. Patients with this problem experience constant hunger, because they have grown adipose tissue require food.
Obesity can cause heart disease, sleep apnea, infertility and diabetes.
Violation of fat metabolism in the body is accompanied by the accumulation of fat not only in the subcutaneous tissue, but also in the blood. As a result of such pathological processes a person develops hyperlipidemia. In this case, blood tests of the patient show an increase in the concentration of cholesterol, triglyceride levels, and low-density lipoproteins in the plasma.
Fatty blood is just as dangerous as the accumulation of fats under the skin. When the amount of lipids in the blood increases, their particles actively penetrate into the walls of the arteries. They are then deposited on the surface of the vessels, thereby giving rise to plaques of atherosclerosis. Such formations gradually grow and can cause blockage of the lumen of blood vessels. In certain cases, the patient may experience a complete cessation of blood flow - a heart attack or stroke.
It is worth noting that sometimes a violation of fat metabolism is manifested by a lack of lipids. In this case, the patient begins to become exhausted and has a lack of fat-soluble vitamins A, D, E and K. A failure also occurs menstrual cycle And reproductive functions. In addition, lipid deficiency causes a lack of essential unsaturated fatty acids, which makes itself felt by hair loss, eczema, inflammatory lesions skin and kidney damage.
About how fat metabolism disorders are corrected, what treatment helps
Patients with metabolic disorders are advised to eliminate risk factors; in addition, they need dietary food. Sometimes only these means of conservative correction are enough to optimize the patient’s condition. However, a person with a disorder metabolic processes Most often, you have to adhere to dietary restrictions throughout your life.
The menu for such patients should include significant amount vegetables, fruits, as well as grains and low-fat dairy products. Physical exercise are selected individually, in addition, patients need to give up smoking, alcohol consumption and protect themselves from stress.
If such measures do not give positive effect, doctors connect drug therapy. In this case, statins can be used, a nicotinic acid and its derivatives, fibrates, antioxidants and sequestrants are sometimes the drugs of choice bile acids. Medicines can only be selected by a doctor, as well as their dosage.
Treatment of fat metabolism disorders with folk remedies
Herbal medicines can be used to treat metabolic disorders. Taking the infusion of fireweed tea gives a good effect. Brew thirty grams of this raw material with half a liter of boiling water, bring the medicine to a boil and leave for half an hour. Take the resulting composition seventy milliliters four times a day.
You can also brew forty grams of plantain leaves with two hundred milliliters of boiling water. Leave covered for half an hour, then strain and take thirty milliliters about twenty minutes before meals three times a day.
You can also combine fifteen grams of horsetail with two hundred milliliters of boiling water. Leave covered for half an hour, then strain. Take fifty milliliters four times a day.
If you suspect the development of metabolic disorders, you should seek doctor's help.
Lipid disorders
Lipids are substances of heterogeneous chemical composition. The human body contains a variety of lipids: fatty acids, phospholipids, cholesterol, triglycerides, steroids, etc. The human need for fats ranges from 80-100 g per day.
Functions of lipids
Structural: Lipids form the basis of cell membranes.
Regulatory.
† Lipids regulate membrane permeability, their colloidal state and fluidity, the activity of lipid-dependent enzymes (for example, adenylate and guanylate cyclases, Na + , K + -ATPase, Ca 2+ -ATPase, cytochrome oxidase), the activity of membrane receptors (for example, for catecholamines, acetylcholine , insulin, cytokines).
† Individual lipids - biologically active substances (for example, Pg, leukotrienes, platelet activating factor, steroid hormones) - regulate the functions of cells, organs and tissues.
Energy supply. Lipids are one of the main sources of energy for striated muscles, liver, kidneys and an additional source of energy for nervous tissue.
Protective. Included subcutaneous tissue lipids form a buffer
a layer that protects soft tissues from mechanical stress.
Insulating. Lipids create a thermally insulating layer in the surface tissues of the body and an electrically insulating sheath around nerve fibers.
Typical forms of pathology
Standard forms pathologies of lipid metabolism are presented in Fig. 10–1.
Rice. 10–1. Typical forms of lipid metabolism pathology.
Depending on the level of lipid metabolism disorders, the following disorders are distinguished:
† Digestion and absorption of lipids in the gastrointestinal tract (for example, as a result of deficiency of pancreatic lipases, impaired bile formation and excretion, disorders of cavity and “membrane” digestion).
† Transmembrane transfer of lipids from the intestine to the blood and their utilization by cells (for example, with enteritis, circulatory disorders in the wall of the small intestine).
† Metabolism of lipids in tissues (for example, with a defect or deficiency of lipases, phospholipases, LPLase).
Depending on the clinical manifestations, obesity, exhaustion, dyslipoproteinemia, lipodystrophy and lipidosis are distinguished.
Obesity
The normal content of adipose tissue in men is 15–20% of body weight, in women - 20–30%.
Obesity is the excessive (pathological) accumulation of fat in the body in the form of triglycerides. At the same time, body weight increases by more than 20–30%.
According to WHO experts, in developed European countries, from 20 to 60% of the population are overweight, in Russia - about 60%.
In itself, an increase in the mass of adipose tissue does not pose a danger to the body, although it reduces its adaptive capabilities. However, obesity increases the risk of ischemic heart disease (1.5 times), atherosclerosis (2 times), hypertension(3 times), diabetes (4 times), as well as some neoplasms (for example, breast, endometrial and prostate cancer).
Types of obesity
The main types of obesity are shown in Fig. 10–2.
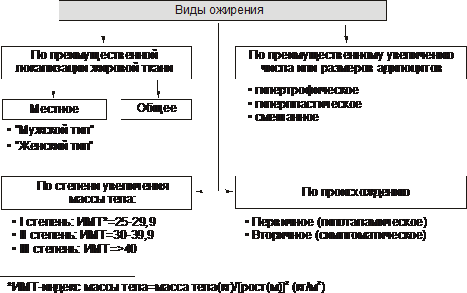
Rice. 10–2. Types of obesity. BMI - body mass index (see text).
Depending on the degree of increase in body weight, three degrees of obesity are distinguished. In this case, the concept of “ideal body weight” is used.
Various formulas are used to estimate ideal body weight.
† The simplest - index Broca : 100 is subtracted from the height indicator (in cm).
†Body mass index is also calculated using the following formula:
Body weight is considered normal with a body mass index in the range of 18.5–24.9. If these values are exceeded, they are said to be overweight (Table 10–1).
Table 10–1. Obesity levels
Note. BMI - body mass index
Based on the predominant localization of adipose tissue, obesity is distinguished between general (uniform) and local (local lipohypertrophy). Types of local obesity:
† Female type (gynoid) - excess subcutaneous fat mainly in the hips and buttocks.
† Male type (android) - accumulation of fat in the abdominal area.
Based on the predominant increase in the number or size of fat cells, the following are distinguished:
† Hyperplastic obesity (due to a predominant increase in the number of adipocytes). It is more resistant to treatment and in severe cases requires surgery to remove excess fat.
† Hypertrophic (due to a predominant increase in the mass and size of adipocytes). It is more often observed after 30 years.
† Hyperplastic-hypertrophic (mixed). It is often detected in childhood.
According to genesis, primary obesity and its secondary forms are distinguished.
† Primary (hypothalamic) obesity is the result of disorders of the fat metabolism regulation system (lipostat) - an independent disease of neuroendocrine genesis.
† Secondary (symptomatic) obesity is a consequence of various disorders in the body, causing:
‡ reduction in energy consumption (and therefore the consumption of triglycerides in adipose tissue),
‡ activation of lipid synthesis - lipogenesis (observed in a number of diseases, for example, diabetes, hypothyroidism, hypercortisolism).
Causes of obesity
The cause of primary obesity is a dysfunction of the adipocyte-hypothalamus system. This is the result of a deficiency and/or insufficiency of the effects of leptin (by suppressing the production of neuropeptide Y by hypothalamic neurons, which increases appetite and hunger).
Secondary obesity develops due to excess calorie intake and P reduced level of energy consumption of the body. Energy consumption depends on the degree of activity (primarily physical) and a person’s lifestyle. Insufficient physical activity is one of the important reasons obesity.
Pathogenesis of obesity
There are neurogenic, endocrine and metabolic mechanisms of obesity.
Neurogenic variants of obesity
Neurogenic (centrogenic and hypothalamic) mechanisms of obesity are presented in Fig. 10–3.
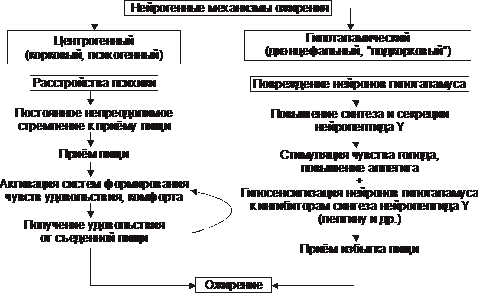
Rice. 10–3. Neurogenic mechanisms of obesity.
† Centrogenic(cortical, psychogenic) mechanism - one of the variants of eating disorder (the other two: anorexia nervosa and bulimia). Reason: various mental disorders, manifested by a constant, sometimes irresistible desire to eat food. Possible mechanisms:
‡ activation of serotonergic, dopaminergic, opioidergic and other systems involved in the formation of feelings of pleasure and comfort;
‡ perception of food as a strong positive stimulus (doping), which further activates these systems - the vicious circle of the centrogenic mechanism of obesity development closes.
† Hypothalamic(diencephalic, subcortical) mechanism. Its cause is damage to the neurons of the ventromedial and paraventricular nuclei of the hypothalamus (for example, after a concussion, with encephalitis, craniopharyngioma, tumor metastases in the hypothalamus). The most important links in pathogenesis:
‡ Spontaneous (without an identified reason) increase in the synthesis and secretion of neuropeptide Y by neurons of the posterolateral ventral nucleus of the hypothalamus.
‡ Damage or irritation of neurons in the above-mentioned nucleus also stimulates the synthesis and secretion of neuropeptide Y and reduces sensitivity to factors that inhibit the synthesis of neuropeptide Y (mainly leptin).
§ Neuropeptide Y stimulates hunger and increases appetite.
§ Leptin suppresses the formation of the appetite stimulant - neuropeptide Y.
‡ Disruption of the participation of the hypothalamus in the formation of the feeling of hunger. This feeling is formed with a decrease in GPC, contraction of the stomach muscles during the evacuation of food and its emptying (feeling of food discomfort - “sucking in the pit of the stomach”). Information from peripheral sensory nerve endings is integrated in the nerve nuclei of the hypothalamus, responsible for eating behavior.
‡ As a result of the above processes, the production of neurotransmitters and neuropeptides that form a feeling of hunger and increase appetite (GABA, dopamine, - endorphin, enkephalins) and/or neurotransmitters and neuropeptides that form a feeling of satiety and inhibit eating behavior (serotonin, norepinephrine, cholecystokinin, somatostatin) is enhanced ).
Endocrine variants of obesity
The endocrine mechanisms of obesity - leptin, hypothyroid, adrenal and insulin - are presented in Fig. 10–4.
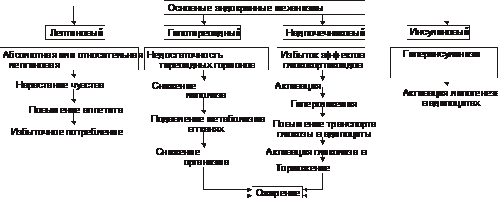
Rice. 10–4. Pathogenesis of obesity.
† Leptin mechanism - leading in the development of primary obesity.
‡ Leptin formed in fat cells. It reduces appetite and increases energy expenditure by the body. The level of leptin in the blood directly correlates with the amount of white adipose tissue. Many cells have leptin receptors, including neurons of the ventromedial nucleus of the hypothalamus. Leptin suppresses the formation and release of neuropeptide Y by the hypothalamus.
‡ NeuropeptideY creates a feeling of hunger, increases appetite, reduces the body's energy consumption. There is a kind of negative feedback between the hypothalamus and adipose tissue: excess food intake, accompanied by an increase in adipose tissue mass, leads to increased secretion of leptin. This (by inhibiting the production of neuropeptide Y) reduces the feeling of hunger. However, in obese people this regulatory mechanism may be impaired, for example, due to increased leptin resistance or mutation of the leptin gene.
‡ Lipostat. The leptin-neuropeptide Y circuit ensures the maintenance of the mass of body adipose tissue - lipostat (or the body’s set point in relation to the intensity of energy metabolism). In addition to leptin, the lipostat system includes insulin, catecholamines, serotonin, cholecystokinin, and endorphins.
† Hypothyroid mechanism obesity is the result of insufficient effects of iodine-containing thyroid hormones. This reduces the intensity of lipolysis, the rate of metabolic processes in tissues and the body's energy costs.
† Adrenal(glucocorticoid, cortisol) mechanism obesity is activated due to hyperproduction of glucocorticoids in the adrenal cortex (for example, during disease or syndrome Itsenko ‑Cushing ). Under the influence of excess glucocorticoids, gluconeogenesis is activated (due to this, hyperglycemia develops), glucose transport into adipocytes, and glycolysis (lipolytic reactions are inhibited and triglycerides accumulate).
† Insulin mechanism The development of obesity develops as a result of direct activation of lipogenesis in adipose tissue by insulin.
† Other mechanisms. Obesity can also develop with other endocrinopathies (for example, with a deficiency of growth hormone and gonadotrophic hormones). The mechanisms of obesity development in these conditions are described in Chapter 27, “Endocrinopathies”).
Metabolic mechanisms of obesity
†Carbohydrate reserves in the body are relatively small. They are approximately equal to their daily intake with food. In this regard, a mechanism for saving carbohydrates has been developed.
†As the proportion of fat in the diet increases, the rate of carbohydrate oxidation decreases. This is evidenced by a corresponding decrease in the respiratory quotient (the ratio of the rate of CO 2 formation to the rate of O 2 consumption).
† If this does not happen (if the mechanism of inhibition of glycogenolysis is disrupted under conditions high concentration fats in the blood), a mechanism is activated that increases appetite and increases food intake, aimed at providing the required amount of carbohydrates in the body.
†Under these conditions, fats accumulate as triglycerides. Obesity develops.
Exhaustion
Wasting and cachexia are pathological decreases in adipose tissue mass below normal. At the same time, the mass of muscle and connective tissue decreases significantly.
With exhaustion, the deficit of adipose tissue can be 20–25% or more (with a body mass index below 20 kg/m2), and with cachexia - below 50%.
Causes and types of exhaustion and cachexia
There are endogenous and exogenous causes of exhaustion.
Exogenous causes
† Forced or conscious full or partial fasting (in the latter case, most often for the purpose of losing weight).
‡ Complete fasting is a condition in which the body does not receive food (for example, in its absence, refusal to eat, inability to eat).
‡ Incomplete fasting is a condition characterized by a significant deficiency of plastic substances and calories in food (for example, with inadequate quantitative and qualitative nutrition, homogeneous food, vegetarianism).
† Low calorie food that does not replenish the body’s energy costs.
Endogenous causes
Depletion of endogenous origin is divided into primary and secondary.
† The causes of primary (hypothalamic, diencephalic) exhaustion are discussed in Fig. 10–5.
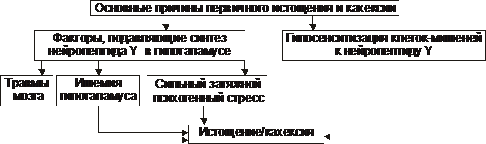
Rice. 10–5. The main causes of primary wasting and cachexia.
† The causes of secondary (symptomatic) exhaustion are shown in Fig. 10–6.
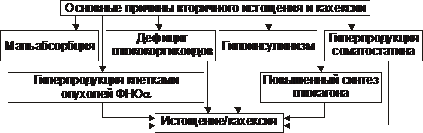
Rice. 10–6. The main causes of secondary wasting and cachexia.
Pathogenesis of wasting and cachexia
Exogenous wasting and cachexia. The absence or significant shortage of food products leads to the development of a chain of sequential and interdependent processes, discussed in Fig. 10–7.
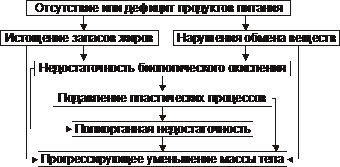
Rice. 10–7. The main links in the pathogenesis of exogenous exhaustion and cachexia.
Primary endogenous forms exhaustion and cachexia. The hypothalamic, cachectic and anorexic forms are of greatest clinical importance.
† Hypothalamic form
In the hypothalamic (diencephalic, subcortical) form of exhaustion and cachexia, there is a decrease or cessation of synthesis and release of peptide Y into the blood by hypothalamic neurons. This leads to the sequential processes shown in Fig. 10–8.
![]()
Rice. 10–8. The main links of the hypothalamic mechanism of exhaustion and cachexia.
† Cachectin form
The pathogenesis of cachectin, or cytokine, form of wasting and cachexia is discussed in Fig. 10–9.
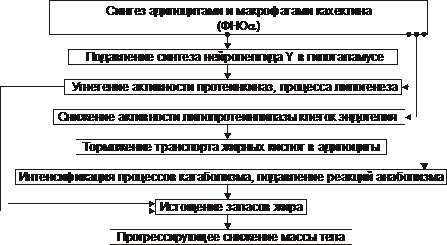
Rice. 10–9. The main links of the cachectin mechanism of exhaustion and cachexia.
† Anorexic form
The main links in the pathogenesis of the anorexic form of exhaustion and cachexia are presented in Fig. 10–10.

Rice. 10–10. The main links of the anorexic mechanism of exhaustion and cachexia.
‡ Individuals who are predisposed to developing anorexia have a critical attitude towards their body (perceived as having overweight) causes the development of neuropsychiatric disorders. This leads to prolonged episodes of food refusal. It is most often observed in teenage girls and girls under 16–18 years of age.
‡ With repeated and emotionally negative stress reactions, excessive formation of serotonin and cholecystokinin, which suppress appetite, is observed.
‡ Further course of the process can lead to the implementation of the effects of neuropeptide Y and cachectin. These factors most likely underlie the pathogenesis of anorexia nervosa. With a prolonged course of the process, a pronounced decrease in body weight develops, up to cachexia.
Secondary endogenous forms exhaustion and cachexia are important, often the main, symptoms of other pathological conditions and diseases (Fig. 10–11).
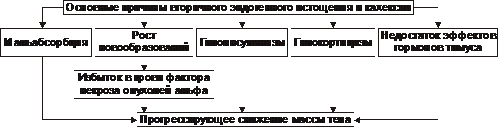
Rice. 10–11. The main causes of secondary endogenous wasting and cachexia.
Lipodystrophy
Lipodystrophy is a condition characterized by generalized or local loss of adipose tissue, less commonly by its excessive accumulation in the subcutaneous tissue. The causes of lipodystrophies are varied and not always known, from mutations of various genes (for example, lamins) to post-injection complications. There is a large group of hereditary and congenital lipodystrophy syndromes, some of them are discussed in the article “Lipodystrophies” (the “Terms Reference” appendix on the CD).
Lipidoses
Lipidoses are a typical form of lipid metabolism disorder, characterized by metabolic disorders of various lipids (for example, sphingolipidoses, gangliosidoses, mucolipidoses, adrenoleukodystrophy, leukodystrophy, lipofuscinosis, cerebrosidosis) in cells (parenchymal lipidoses), fatty tissue (obesity, emaciation) or the walls of arterial vessels (atherosclerosis). , arteriosclerosis). These forms of lipidoses are described in this textbook (Chapter 4 “Cell Damage”, in this chapter, as well as in the articles in the Appendix “Reference Book of Terms” on the CD).
Dyslipoproteinemia
Dislipoproteinemia is a condition characterized by a deviation from the norm in the content, structure and ratio of various drugs in the blood. Drug metabolism disorders are the main link in the pathogenesis of atherosclerosis, ischemic heart disease, pancreatitis and other diseases.
The nature of the course and clinical manifestations of dislipoproteinemia are determined by:
Hereditary properties of the body (for example, the composition, ratio and level of various drugs; the characteristics of their metabolism).
Environmental factors (for example, a set of food products, dietary features and eating patterns).
The presence (or absence) of concomitant diseases (for example, obesity, hypothyroidism, diabetes, kidney and liver damage).
Characteristics of lipoproteins
Various lipids circulate in the blood plasma. Free fatty acids are transported by albumin, and triglycerides, cholesterol, cholesteryl esters and phospholipids, and a small amount of fatty acids are transported as part of the drug. These spherical particles consist of a hydrophobic core (contains cholesteryl esters and triglycerides) and a hydrophilic shell (contains cholesterol, phospholipids and apolipoproteins). The main characteristics of different drugs are given in table. 10–2.
Table 10–2. Types and main properties of lipoproteins
|
Chylomicrons | |||||
|
Particle size (nm) |
75–1200 | ||||
|
Density (g/cm 3 ) |
0,98–1,006 |
1,006–1,019 |
1,019–1,063 |
1,063–1,210 |
|
|
Compound (%): | |||||
|
Cholesterol | |||||
|
Triglycerides | |||||
|
Phospholipids | |||||
|
ApoLP |
B48, AI, AII, AIV, CI, CII, CIII, E |
B100, CI, CII, CIII, E |
AI, AII, AIV, CI, CII, CIII, E |
||
|
Source |
Small intestine, food lipids |
Liver, small intestine |
VLDL, LPPP |
Small intestine, liver |
|
|
Atherogenicity |
Not proven |
Not proven |
Antiatherogenic |
||
Apolipoproteins ensure the preservation of the ordered structure of drug micelles, the interaction of drugs with cell receptors, and the exchange of components between drugs. Detailed characteristics apoLP and their defects are given in the article “Defects of apolipoproteins” (see the Appendix “Reference of Terms” on the CD).
Atherogenicity of lipoproteins
LPs are divided into atherogenic and antiatherogenic (Fig. 10–12).

Rice. 10–12. Types of lipoproteins depending on their atherogenicity.
The antiatherogenic effect of HDL is determined by their following properties:
† The ability to remove excess cholesterol from the plasma membrane of cells, including the vascular endothelium, and transfer it to the liver, where cholesterol is removed with bile.
† Higher affinity of HDL for apoLP E and apoLP B receptors compared to LDL. This is determined high content apoLP E to HDL. As a result, HDL prevents cells from taking up cholesterol-laden particles.
Assessment of the potential atherogenicity of blood lipids is carried out by calculating the cholesterol atherogenicity coefficient:
Normally, the cholesterol atherogenic coefficient does not exceed 3.0. As this value increases, the risk of developing atherosclerosis increases.
Types of dyslipoproteinemia
The main types of dislipoproteinemia are shown in Fig. 10–13.
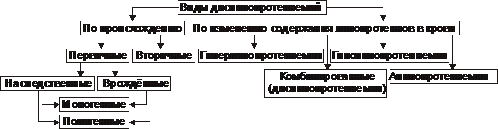
Rice. 10–13. Types of dislipoproteinemia.
More than 30% of primary dislipoproteinemias are inherited forms of pathology (both monogenic and polygenic with multifactorial genesis).
About 70% of dyslipoproteinemias are considered acquired. Secondary (acquired) dyslipoproteinemias are symptoms of other diseases. They accompany many human diseases (Table 10–3).
Table 10–3. The most common pathological processes leading to the development of secondary dislipoproteinemia
|
Disease |
Development mechanism |
|
|
Diabetes |
I, IV, V |
Decreased LPLase activity, excess flow of fatty acids into the liver, increased VLDL synthesis |
|
Impaired lipid secretion |
||
|
Primary cirrhosis of the liver |
Impaired drug synthesis |
|
|
Nephrotic syndrome |
II, IV, V |
Increased formation of lipoproteins and triglycerides |
|
Hypothyroidism |
II, IV | |
|
Pituitary insufficiency |
Reduced lipid catabolism |
|
|
Chronic alcoholism |
IV, V |
Decreased LPLase activity, increased lipid synthesis |
Various hereditary defects, as well as acquired pathological processes and diseases often lead to similar changes in the content and profile of various drugs. In this regard, fine differentiation of their origin is required, allowing for their effective treatment.
Hyperlipoproteinemia
Hyperlipoproteinemia is a condition characterized by a disorder of the formation, transport and metabolism of drugs and manifested by a persistent increase in the content of cholesterol and/or triglycerides in the blood plasma.
Classification
In 1967, Fredrickson and co-authors developed a classification of hyperlipoproteinemias (hyperlipidemias). The basis was based on content data total cholesterol and triglycerides in blood plasma, as well as features of the distribution of drug fractions during their electrophoresis and ultracentrifugation. On this basis, five types of hyperlipoproteinemia have been identified. This classification was later revised by WHO specialists (Table 10-4).
Violations and their causes in alphabetical order:
lipid metabolism disorder -
Whole line diseases caused by lipid metabolism disorder. The most important among them are atherosclerosis and obesity. Diseases of cardio-vascular system, as a consequence of atherosclerosis, occupy first place in the structure of mortality in the world. One of the most common manifestations of atherosclerosis is damage coronary vessels hearts. The accumulation of cholesterol in the walls of blood vessels leads to the formation of atherosclerotic plaques. They, increasing in size over time, can block the lumen of the vessel and interfere with normal blood flow. If, as a result, blood flow is disrupted in coronary arteries, then it arises angina or myocardial infarction. Predisposition to atherosclerosis depends on the concentration of transport forms of blood lipids - plasma alpha-lipoproteins.
What diseases cause lipid metabolism disorders:
The accumulation of cholesterol (CH) in the vascular wall occurs due to an imbalance between its entry into the vascular intima and its exit. As a result of this imbalance, cholesterol accumulates there. In the centers of cholesterol accumulation, structures are formed - atheromas. The best known are two factors that cause lipid metabolism disorders.
1. Firstly, these are changes in LDL particles (glycosylation, lipid peroxidation, phospholipid hydrolysis, apo B oxidation). Therefore, they are captured by special cells - “scavengers” (mainly macrophages). The uptake of lipoprotein particles by “garbage” receptors proceeds uncontrollably. Unlike apo B/E-mediated endocytosis, this does not cause regulatory effects aimed at reducing the entry of cholesterol into the cell, described above. As a result, macrophages become overloaded with lipids, lose their waste absorption function, and turn into foam cells. The latter are retained in the wall blood vessels and begin to secrete growth factors that accelerate cell division. Atherosclerotic cell proliferation occurs.
2. Secondly, it is the ineffective release of cholesterol from the endothelium vascular wall circulating in blood HDL.
Factors influencing increased level LDL in humans
Gender - higher in men than in premenopausal women and lower than in postmenopausal women
- Aging
- Saturated fats in diet
- High consumption cholesterol
- Diet low in coarse fiber foods
- Alcohol consumption
- Pregnancy
- Obesity
- Diabetes
- Hypothyroidism
- Cushing's disease
- Uremia
- Nephrosis
- Hereditary hyperlipidemia
Lipid metabolism disorders (dyslipidemia), characterized primarily by increased content in the blood cholesterol and triglycerides are the most important factors risk of atherosclerosis and related diseases of the cardiovascular system. Plasma concentrations of total cholesterol (TC) or its fractions closely correlate with morbidity and mortality from coronary artery disease and other complications of atherosclerosis. Therefore, the characteristics of lipid metabolism disorders are prerequisite effective prevention cardiovascular diseases.
Lipid metabolism disorders can be primary or secondary and are characterized only by an increase in cholesterol (isolated hypercholesterolemia), triglycerides (isolated hypertriglyceridemia), triglycerides and cholesterol (mixed hyperlipidemia).
The primary disorder of lipid metabolism is determined by single or multiple mutations of the corresponding genes, as a result of which there is overproduction or impaired utilization of triglycerides and LDL cholesterol or overproduction and impairment of HDL clearance.
Primary lipid metabolism disorder can be diagnosed in patients with clinical symptoms these violations, with early start atherosclerosis (up to 60 years), in persons with a family history of atherosclerosis or with an increase in serum cholesterol > 240 mg/dL (> 6.2 mmol/L).
Secondary lipid metabolism disorder occurs, as a rule, in the population of developed countries as a result of sedentary lifestyle life, consumption of food containing large amounts of cholesterol, saturated fatty acids.
Other causes of secondary lipid metabolism disorders may be:
1. Diabetes mellitus.
2. Alcohol abuse.
3. Chronic renal failure.
4. Hyperthyroidism.
5. Primary biliary cirrhosis.
6. Taking certain medications (beta blockers, antiretroviral drugs, estrogens, progestins, glucocorticoids).
Hereditary disorders of lipid metabolism:
A small number of people experience hereditary disorders lipoprotein metabolism, manifested in hyper- or hypolipoproteinemia. They are caused by a violation of the synthesis, transport or breakdown of lipoproteins.
In accordance with generally accepted classification, there are 5 types of hyperlipoproteinemia.
1. The existence of type 1 is due to insufficient LPL activity. As a result, chylomicrons are removed from the bloodstream very slowly. They accumulate in the blood, and VLDL levels are also higher than normal.
2. Type 2 hyperlipoproteinemia is divided into two subtypes: 2a, characterized by a high content of blood LDL, and 2b (increase in LDL and VLDL). Type 2 hyperlipoproteinemia is manifested by high, and in some cases very high, hypercholesterolemia with the development of atherosclerosis and coronary disease hearts. The content of triacylglycerols in the blood is within normal limits (type 2a) or moderately increased (type 2b). Hyperlipoproteinemia type 2 is characteristic of serious illness- hereditary hypercholesterolemia affecting young people. In the case of the homozygous form it ends fatal V at a young age from myocardial infarction, strokes and other complications of atherosclerosis. Hyperlipoproteinemia type 2 is widespread.
3. With type 3 hyperlipoproteinemia (dysbetalipoproteinemia), the conversion of VLDL to LDL is impaired, and pathological floating LDL or VLDL appears in the blood. The content of cholesterol and triacylglycerols in the blood is increased. This type is quite rare.
4. With type 4 hyperlipoproteinemia, the main change is an increase in VLDL. As a result, the content of triacylglycerols in the blood serum is significantly increased. Combined with atherosclerosis of the coronary vessels, obesity, diabetes mellitus. It develops mainly in adults and is very common.
5. Type 5 hyperlipoproteinemia – an increase in the blood serum content of cholesterol and VLDL, associated with moderate decreased activity lipoprotein lipases. LDL and HDL concentrations are below normal. The content of triacylglycerols in the blood is increased, while the concentration of cholesterol is within normal limits or moderately increased. Occurs in adults, but widespread does not have.
Typing of hyperlipoproteinemia is carried out in the laboratory based on the study of the content of various classes of lipoproteins in the blood using photometric methods.
The cholesterol level in HDL is more informative as a predictor of atherosclerotic lesions of the coronary vessels. Even more informative is the coefficient reflecting the ratio of atherogenic to antiatherogenic drugs.
The higher this coefficient, the more danger occurrence and progression of the disease. In healthy individuals, it does not exceed 3-3.5 (in men it is higher than in women). U patients with ischemic heart disease it reaches 5-6 or more units.
Is diabetes a disease of lipid metabolism?
The manifestations of lipid metabolism disorders are so pronounced in diabetes that diabetes is often called more of a disease lipid than carbohydrate metabolism. The main disorders of lipid metabolism in diabetes are increased lipid breakdown, increased formation of ketone bodies and decreased synthesis of fatty acids and triacylglycerols.
U healthy person usually 50% of incoming glucose is broken down by CO2 and H2O; about 5% is converted to glycogen, and the rest is converted to lipids in fat stores. In diabetes, only 5% of glucose is converted into lipids, while the amount of glucose decomposed into CO2 and H2O also decreases, and the amount converted into glycogen changes slightly. The result of impaired glucose consumption is an increase in the level of glucose in the blood and its removal in the urine. Intracellular glucose deficiency leads to a decrease in the synthesis of fatty acids.
In patients not receiving treatment, there is an increase in the plasma content of triacylglycerols and chylomicrons and the plasma is often lipemic. An increase in the level of these components causes a decrease in lipolysis in fat depots. Decreased lipoprotein lipase activity further contributes to decreased lipolysis.
Lipid peroxidation
Features of lipids cell membranes is their significant unsaturation. Unsaturated fatty acids are easily subject to peroxide destruction - LPO (lipid peroxidation). The membrane response to damage is therefore called “peroxide stress”.
LPO is based on the free radical mechanism.
Free radical pathology is smoking, cancer, ischemia, hyperoxia, aging, diabetes, i.e. In almost all diseases, uncontrolled formation occurs free radicals oxygen and intensification of LPO.
The cell has systems to protect itself from free radical damage. The antioxidant system of cells and tissues of the body includes 2 links: enzymatic and non-enzymatic.
Enzymatic antioxidants:
- SOD (superoxide dismutase) and ceruloplasmin, involved in the neutralization of oxygen free radicals;
- catalase, which catalyzes the decomposition of hydrogen peroxide; the glutathione system, which ensures the catabolism of lipid peroxides, peroxide-modified nucleotides and steroids.
Even a short-term lack of non-enzymatic antioxidants, especially antioxidant vitamins (tocopherol, retinol, ascorbate), leads to persistent and irreversible damage to cell membranes.
Which doctors should you contact if a lipid metabolism disorder occurs:
Have you noticed a lipid metabolism disorder? Do you want to know more detailed information or do you need an inspection? You can make an appointment with a doctor– clinic Eurolab always at your service! The best doctors they will examine you and study you external signs and will help you identify the disease by symptoms, advise you and provide necessary help. you also can call a doctor at home. Clinic Eurolab open for you around the clock.symptoms of diseases and do not realize that these diseases can be life-threatening. There are many diseases that at first do not manifest themselves in our body, but in the end it turns out that, unfortunately, it is too late to treat them. Each disease has its own specific symptoms, characteristic external manifestations- so called symptoms of the disease. Identifying symptoms is the first step in diagnosing diseases in general. To do this, you just need to do it several times a year. be examined by a doctor to not only prevent terrible disease, but also support healthy mind in the body and the organism as a whole.
If you want to ask a doctor a question, use the online consultation section, perhaps you will find answers to your questions there and read self care tips. If you are interested in reviews about clinics and doctors, try to find the information you need on. Also register on medical portal Eurolab to stay up to date latest news and information updates on the website, which will be automatically sent to you by email.
The symptom chart is for educational purposes only. Do not self-medicate; For all questions regarding the definition of the disease and methods of its treatment, consult your doctor. EUROLAB is not responsible for the consequences caused by the use of information posted on the portal.
If you are interested in any other symptoms of diseases and types of disorders, or you have any other questions or suggestions, write to us, we will definitely try to help you.
