Non-rheumatic myocarditis. Anatomical features of the structure of the heart
§ in the group of patients at moderate risk - ampicillin or amoxicillin 2.0 g intravenously per 0.5–1 hour before intervention (or amoxicillin 2.0 g orally);
If you have an allergic reaction to benzylpenicillin:
§ in a group of patients high risk– vancomycin 1.0 g more than 1–2 hours before the procedure + gentamicin 1.5 mg/kg intramuscularly;
§ in the group of patients at moderate risk - vancomycin 1.0 g for more than 1–2 hours before the procedure without gentamicin.
Not rheumatic myocarditis
Myocarditis is an acute, subacute or chronic inflammatory lesion of the myocardium, predominantly of infectious and (or) immune etiology, which can manifest itself with general inflammatory, cardiac symptoms (cardialgia, ischemia, heart failure, arrhythmia, sudden death) or occur latently.
Myocarditis is characterized by great variability clinical picture; It is often combined with pericarditis (the so-called myopericarditis); simultaneous involvement of the endocardium in the inflammatory process is also possible. For the convenience of distinguishing between rheumatic and other variants of myocarditis, the term “non-rheumatic myocarditis” is used.
Myocarditis, accompanied by dilation of the heart cavities and myocardial contractile dysfunction, is included in the American Classification of Primary Cardiomyopathies (2006) under the name “inflammatory cardiomyopathy.” This term was proposed to distinguish among patients with severe dilatation of the heart chambers (DCM), those whose disease is based on an inflammatory process that is subject to specific treatment (as opposed to patients with genetic DCM).
Myocarditis can be an independent condition or a component of another disease (for example, systemic scleroderma, SLE, IE, systemic vasculitis, etc.).
Epidemiology
The true prevalence of myocarditis is unknown due to difficulties in verifying the diagnosis. According to some reports, the frequency
the diagnosis of “myocarditis” in cardiology hospitals is about 1%, at autopsy in young people who died suddenly or as a result of injuries - 3-10%, in infectious diseases hospitals - 10-20%, in rheumatology departments - 30-40%.
Classification
The classification of myocarditis, proposed in 2002 by N. R. Paleev, F. N. Paleev and M. A. Gurevich, is based mainly on the etiological principle and is presented in a slightly modified form.
1. Infectious and infectious-immune.
2. Autoimmune:
rheumatic;
for diffuse connective tissue diseases (SLE, rheumatoid arthritis, dermatomyositis, etc.);
with vasculitis ( periarteritis nodosa, Takayasu's disease, Kawasaki's disease, etc.);
with IE;
for other autoimmune diseases (sarcoidosis, etc.);
hypersensitive (allergic), including medicinal.
3. Toxic (uremic, thyrotoxic, alcoholic).
4. Radiation.
5. Burn.
6. Transplantation.
7. Unknown etiology (giant cell, Abramov-Fiedler and
The etiological agent of infectious myocarditis can be bacteria (brucella, clostridia, corynebacteria diphtheria, gonococci, Haemophilus influenzae, legionella, meningococci, mycobacteria, mycoplasma, streptococci, staphylococci), rickettsia (Rocky Mountain fever, cholera fever, tsutsugamushi fever, rash typhus), spirochetes (Borrelia, Leptospira, Treponema pallidum), protozoa (amoebas, Leishmania, Toxoplasma, trypanosomes that cause Chagas disease), fungi and helminths.
The most common causes of infectious myocarditis are adenoviruses, enteroviruses (Coxsackie group B, ECHO), herpes viruses (cytomegalovirus, Epstein-Barr virus,
herpes type 6, herpes zoster), HIV, influenza and parainfluenza viruses, parvovirus B19, as well as hepatitis B, C viruses, mumps, polio, rabies, rubella, measles, etc. The development of a mixed infection (two viruses, a virus and a bacterium, etc.) is possible.
Myocarditis in infectious diseases may not have a large clinical significance, develop as part of multiple organ damage (typhoid fever, brucellosis, borreliosis, syphilis, HIV infection, hepatitis C virus infection, cytomegalovirus) or come to the fore in the clinical picture and determine the prognosis (myocarditis with diphtheria, enterovirus infection, other viral myocarditis and Chagas disease).
In infectious (especially viral) myocarditis, the development of autoimmune reactions is typical, and therefore it can be difficult to distinguish between infectious and infectious-immune myocarditis.
According to the flow, there are three variants of myocarditis:
1. acute – acute onset, pronounced clinical signs, increased body temperature, significant changes in laboratory (acute-phase) parameters;
2. subacute – gradual onset, protracted course (from a month to six months), less severe acute-phase indicators;
3. chronic – long-term course (more than six months), alternating exacerbations and remissions.
According to the severity of the course, the following variants of myocarditis are distinguished:
1. mild – mild, occurs with minimal symptoms;
2. moderate severity - moderately expressed, symptoms are more distinct, slightly pronounced signs of heart failure are possible);
3. severe – pronounced, with signs of severe heart failure;
4. fulminant (fulminant), in which extremely severe heart failure requires immediate hospitalization in the department intensive care and intensive care, develops within a matter of hours from the onset of the disease and often ends in death.
According to the prevalence of the lesion, the following are distinguished:

variants of myocarditis:
1. focal - usually does not lead to the development of heart failure, can only manifest as rhythm and conduction disturbances, and presents significant difficulties for diagnosis;
2. diffuse.
Etiology
The presented classification implies an extreme variety of factors leading to the development of myocarditis. The most common cause (up to 50% of cases) of myocarditis is infectious diseases, especially viral ones.
Pathogenesis
Various etiological factors cause myocardial damage and the release (unmasking or exposure) of its antigens. The immunocompetent system determines the production of antimyocardial antibodies, which are involved in the formation immune complexes leading to further myocardial damage. Along with this, a delayed-type reaction develops, as a result of which T-lymphocytes become aggressive towards the myocardium.
Thus, its damage occurs through the following mechanisms:
1. direct myocardiocytolytic effect due to myocardial invasion and replication of the pathogen;
2. cellular damage from circulating toxins;
3. nonspecific cellular damage as a result of generalized inflammation;
4. cellular damage due to the production of factors by specific cells or the humoral immune system in response to an agent.
These mechanisms influence the timing of the onset of myocarditis (early or long-term period development of an infectious disease.
Clinical picture
The clinical picture of myocarditis is very diverse and is largely determined not only by the etiological factor, but also by the reactivity of the body, as well as the genetically programmed characteristics of the immune response. With an adequate response of the body to the influence of an infectious agent, myocarditis may be limited to the infectious phase and result in complete recovery. If the immune system is unable to completely eliminate the pathogen, its long-term persistence in the myocardium occurs, accompanied by autoimmune reactions, which leads to chronic and, as a rule, diffuse inflammation, in which it is not easy to establish a connection between the disease and a previous infection or exposure to another etiological factor.
At the first stage diagnostic searchOf greatest importance is the identification of complaints indicating possible heart damage and their connection with the previous infection. The disease occurs more often in older people 20–40 years, but can develop at any age, including in elderly patients, in combination with other heart diseases (CHD, hypertension), which makes diagnosis difficult. However, the appearance of symptoms of myocarditis in elderly patients can be interpreted as ischemic heart disease without sufficient grounds.
Patients with myocarditis often complain of various kinds painful sensations in the area of the heart. An essential sign (as a rule) is their non-anginal nature: the pain is long-lasting, not associated with physical activity, has a wide variety of character (stabbing, aching, dull, burning), and at low intensity can be described by the patient as discomfort, discomfort in the heart area. However, typical anginal pain may also occur, caused by the involvement of small (intramyocardial) vessels in the inflammatory process. Intense pain in the heart area is possible (especially with accompanying inflammation pericardial layers), which may require injection narcotic analgesics and become a source of diagnostic errors - the condition is regarded as MI.
The feeling of palpitations and interruptions are typical for myocarditis and may be its only clinical manifestation; their appearance along with other signs indicates the “interest” of the heart and directs the diagnostic search along the right path. Big role
To make a correct diagnosis, symptoms of heart failure, expressed to varying degrees, play a role: shortness of breath on exertion or at rest, heaviness in the right hypochondrium due to liver enlargement, swelling of the legs, “congestive” cough, decreased urine output. By themselves, these symptoms do not indicate myocarditis, as they occur in various heart diseases, but their presence and combination with other symptoms indicate the severity of damage to the heart muscle. Increased fatigue, weakness, and low-grade fever are quite often observed in patients with myocarditis, but they are to a much greater extent due to post-infectious asthenia.
Thus, the listed symptoms occur in many diseases of cardio-vascular system and they cannot be considered as obligatory clinical signs of myocarditis, but they should be taken into account when the patient consults a doctor, especially after suffering an acute respiratory, intestinal or unclear febrile illness.
The medical history often has crucial in making a diagnosis of myocarditis. In addition to the connection between cardiac symptoms at the onset of the disease (and their exacerbation during the chronic course of the disease) with a previous infection, it is necessary to take into account the severity of the disease, which is not typical for most other heart diseases. At the same time, a long-term chronic course of both mild, latent and severe myocarditis is possible in the absence of an acute onset and a clear connection between the disease and infection, which creates significant difficulties in differential diagnosis. If chronic myocarditis is suspected, the effectiveness of immunosuppressive, anti-inflammatory and (or) antiviral (antibacterial) therapy in the anamnesis is of diagnostic importance.
It is necessary to find out carefully family history(presence of unspecified “heart disease”, unexplained heart failure in relatively young relatives), information about chronic infectious diseases of any localization, about the frequency and severity of common “colds” and ARVI. A history of tonsillitis and chronic tonsillitis require special attention, since, while not always leading to the development of ARF, they often induce non-rheumatic autoimmune myocarditis. Constant professional contact of the patient with infectious pathogens is important (doctors, especially local doctors, infectious and surgical specialists, employees of bacteriological and virological laboratories,
nurses). Finally, when collecting anamnesis, it is necessary to pay attention to signs of systemic immune damage, to information about damage to other organs and systems, which, in combination with myocarditis, may constitute a characteristic picture of a particular infectious or systemic disease.
The amount of information important for making a diagnosis that can be obtained for myocarditis on the second stage of the diagnostic search,
depends on the severity of the disease.
The most significant for the diagnosis of severe myocarditis is the detection of the following symptoms: muffling of the first tone, gallop rhythm, systolic murmur at the apex of the heart, rhythm disturbances (mainly extrasystoles), as well as expansion of the boundaries of the heart. With significant dilatation of the heart chambers, visible pulsation may appear in the precordial region; with concomitant pericarditis, a pericardial friction rub may be heard. However, these symptoms do not have a specific diagnostic value, since they occur in other diseases accompanied by myocardial damage with a decrease in its contractile function. You can also detect symptoms of heart failure in the form of acrocyanosis, jaundice of the skin (as a result of severe congestive liver damage or combined infectious hepatitis), orthopnea, edema, swelling of the jugular veins, shortness of breath, small-bubbly, silent (congestive) wheezing in the lower parts of the lungs, enlarged liver. Naturally, the symptoms of heart failure reflect a decrease in the contractile function of the myocardium, and if the diagnosis of severe myocarditis is confirmed, they will indicate the significant severity of its course and the prevalence of myocardial damage (diffuse myocarditis).
However, at this stage there may be no signs of heart failure. Then we should assume mild course myocarditis (in such cases, the diagnosis will be based on anamnestic data and the results of laboratory and instrumental research methods) or the presence of another disease that occurs with complaints similar to those presented by patients with myocarditis (for example, NCD).
It should be remembered that an enlarged heart and signs of heart failure can appear not only with myocarditis, but also with another group of diseases (for example, with valvular heart defects, ischemic heart disease with the development of a cardiac aneurysm, “storage” diseases involving the myocardium in the process, idiopathic cardiomyopathy) . Due to this
the search for symptoms that reject or confirm the presence of these diseases is very important (naturally, the data obtained must be compared with the anamnesis, and subsequently with the data of laboratory and instrumental research methods).
At the second stage of the diagnostic search, you can detect symptoms of the disease that caused the development of myocarditis (for example, SLE, IE, etc.). Their determination with undoubted signs of myocardial damage will indicate the etiology of myocarditis.
At the third stage of the diagnostic search, it is possible to detect three groups of symptoms:
1. confirming or excluding myocardial damage;
2. indicating the severity of the inflammatory process (nonspecific or immune-based);
3. clarifying the diagnosis of a disease that can lead to the development of myocarditis.
The results of laboratory tests have varying sensitivity and specificity in the diagnosis of forms of myocarditis of different etiologies and should be assessed in conjunction with other data.
Laboratory indicators can be divided into several groups according to their meaning.
1. Indicators to prove inflammatory necrotic damage to the myocardium:
Detection of cardiac troponin I and T in the blood, increased activity of MB-CPK, CPK, LDH (with a violation of the ratio of fractions: LDH-1 › LDH-2), AST and ALT (characteristic only for severe, usually acute, myocarditis);
An increase in the titer of anticardiac antibodies (to various heart antigens) of the IgM class (characteristic of an acute process) and IgG, which can arise and increase after some time from the onset of the disease;
Positive reaction of inhibition of leukocyte migration in the presence of myocardial antigen.
2. Indicators to prove the existence of a past or active infectious disease:
Detection of the genome of cardiotropic viruses and some other pathogens in the blood (by PCR method);
In rare cases of septic myocarditis - positive
blood culture, increased blood procalcitonin levels;
detection of increased titer of antiviral or antibacterial antibodies (IgM or IgG class);
acute phase indicators:
§ increase in the number of neutrophil leukocytes with a shift leukocyte formula to the left (eosinophilia, especially pronounced (more than 1500 cells per 1 ml) makes one think of the hypersensitive (eosinophilic) version of myocarditis as an independent disease or as part of a systemic process);
§ increase in ESR;
§ SRB detection;
§ dysproteinemia (increased contentα2-globulins and
fibrinogen);
3. Indicators that allow you to prove immune disorders, which in themselves are not specific enough, but may reflect disease activity:
Decrease in the number of T-lymphocytes in peripheral blood;
Increased blood levels of Ig classes A and G;
Detection of increased titer of circulating immune complexes (CIC);
Increased concentrations of IL-6, TNF-a and a number of other inflammatory mediators;
The presence in the blood of RF in an increased titer, antibodies to DNA, cardiolipin, and in rare cases, antinuclear factor (ANF).
4. Indicators reflecting the severity of heart failure and liver and kidney dysfunction associated with congestion:
Increased levels of atrial natriuretic factor;
Laboratory signs of cholestasis syndrome, hepatocellular and renal failure.
5. Indicators to confirm the existence of an underlying disease that contributed to the development of myocarditis.
In general, non-rheumatic myocarditis is characterized by the absence or insignificance of laboratory changes. A persistent increase in acute phase parameters in combination with fever requires the exclusion of bacterial myocarditis.
Taking into account the data from all stages of the diagnostic search, the diagnosis
myocarditis can be diagnosed with sufficient convincing. Sometimes, however, it is necessary to use other research methods included in the additional scheme. These methods should not be used in all cases.
Methods for studying central hemodynamics are not essential and mandatory for diagnosing myocarditis. By identifying one or another degree of impairment of the pumping function of the heart, they objectify the severity of heart failure. Along with the dynamic changes indicators of central hemodynamics during treatment make it possible to assess the effectiveness of the therapy.
An ECG, as well as daily Holter ECG monitoring, are required in the diagnosis of myocarditis.
The meaning of the received data may vary.
1. The absence of any changes on the ECG and according to Holter monitoring makes the diagnosis of myocarditis problematic.
2. Changes in the terminal part of the ventricular complex(ST and T waves) are often nonspecific (negative, smoothed or biphasic T waves predominantly in the left precordial leads, rarely resembling coronary leads), but with the simultaneous development of pericarditis, ST segment elevation may appear, which is often regarded as a sign of the most acute phase of myocardial infarction; in addition, typical “ischemic” depression of the ST segment may develop, associated with damage to small coronary arteries.
3. Very characteristic of myocarditis are rhythm disturbances of the most varied nature, which may be the only manifestation of the disease; during an active process, arrhythmias are often polytopic in nature (ventricular and supraventricular extrasystole, AF, atrial flutter (AF), VT, recurrent atrial tachycardia, etc.) and are resistant to antiarrhythmic therapy.
4. Conduction disturbances are also typical, often occurring at different levels - atrioventricular blockade, sinus bradycardia, complete blockade of the left bundle branch (more often develops in severe acute myocarditis; in chronic myocarditis it can occur transitory nature) and etc.
5. With myocarditis, dynamism is noted ECG changes that almost completely disappear after recovery. At the same time on
throughout the day (hours) in patients with myocarditis, there are no dynamic changes in the ECG, unlike the ECG of patients with NCD, in which ECG indicators are characterized by instability even during the registration period. Drug tests (potassium test, test with β-blockers) normalize the altered ECG in patients with NCD; in case of myocarditis, the tests are negative.
6. In the chronic course of myocarditis (usually severe or moderate), changes in the ECG are quite persistent and are caused by the development of myocardial cardiosclerosis. This applies not only to the interval S-T and T wave, but also to disturbances of atrioventricular and (or) intraventricular conduction and rhythm disturbances. A sign of a significant decrease in the mass of the working ventricular myocardium may be a decrease or complete disappearance of R waves in the chest leads (with the formation of QS complexes).
7. Similar changes in the ECG can be observed in other heart diseases (coronary artery disease, acquired heart defects and hypertension). The question of whether ECG changes correspond to a particular disease is decided on the basis of the totality of other symptoms detected at all three stages of the diagnostic search.
An X-ray examination carried out in patients with myocarditis makes it possible to clarify the degree of general enlargement of the heart and its individual chambers. In severe diffuse myocarditis, all parts of the heart are enlarged, there are signs of circulatory disorders in the pulmonary circle in the form of increased pulmonary pattern and expansion of the roots of the lungs. Milder myocarditis is characterized by minimal enlargement of only the left ventricle or normal sizes of the heart chambers. X-ray examination allows us to exclude exudative pericarditis as the cause of heart enlargement, in which a peculiar round shadow of the heart is detected in the absence of pulsation along its outer contour, as well as constrictive pericarditis, which is characterized, although not necessarily, by calcium deposits in the pericardial layers.
EchoCG for myocarditis often has great diagnostic value.
1. In the presence of an enlarged heart, EchoCG data can exclude cardiomegaly as the cause valve defects, post-infarction cardiac aneurysm, exudative pericarditis, HCM.
Detection of significant thickening of the walls of the left ventricle with a decrease in its contractile function requires the exclusion of storage diseases (amyloidosis, Fabry disease, etc.) and contradicts the diagnosis of myocarditis.
2. The study allows you to more accurately determine the severity of dilatation of various chambers of the heart (primarily the left ventricle). Most important factors in assessing the remodeling of the left ventricle and its contractility, end-diastolic size, diastolic and systolic volumes, ejection fraction (the percentage of blood that is ejected by the ventricle in one systole), systolic pressure in the pulmonary artery. With significant dilatation of the ventricles, relative insufficiency of the mitral and tricuspid valves is also detected. In order to determine the indications for resynchronization therapy, ultrasound assessment the presence and severity of interventricular and intraventricular dyssynchrony (non-simultaneous contraction of different segments).
3. In severe myocarditis, signs of total myocardial hypokinesia are detected (in contrast to local zones of hypokinesia in ischemic heart disease).
4. In patients with AF, as well as a pronounced decrease in left ventricular contractility, intracardiac thrombi can be detected (both in the atria and ventricles).
5. EchoCG can detect signs of non-compact myocardium (it is located inward of the compact layer, has a loose spongy structure, predisposes to intracardiac thrombosis). This disease, as a rule, is genetically determined, is often combined with other heart anomalies and leads to a significant decrease in the contractility of the ventricles of the heart; its detection casts doubt on the diagnosis of myocarditis.
6. Echocardiographic changes characteristic of severe myocarditis are difficult to differentiate from primary (genetic) DCM. Such differentiation is possible by taking into account the entire clinical picture of the disease, and primarily the anamnesis data.
7. EchoCG, unlike most other instrumental studies, can be repeated an unlimited number of times, which makes it possible to objectively assess the condition over time (for example, in severe acute myocarditis, the development of pronounced edema of the walls of the left ventricle with its subsequent regression can be noted).
8. In mild myocarditis, echocardiography does not reveal changes in the size and contractility of the heart chambers. Possible definition
minimal signs of damage to the myocardium and pericardium (subclinical valve regurgitation, thickening of the pericardial layers, a small amount of fluid in the pericardial cavity, etc.).
Complex laboratory examinations, ECG, Holter monitoring and EchoCG are mandatory in the diagnosis of myocarditis; however, often these methods are not enough. To verify the diagnosis, they additionally use various methods(radiography, ultrasound, CT) and determine foci of chronic infection of non-cardiac localization, primarily lesions of the ENT organs. Consultation with an otorhinolaryngologist with a culture from the tonsils (or pharynx) is mandatory when examining patients with suspected myocarditis.
Radionuclide methods (myocardial scintigraphy) make it possible to prove the presence of foci of cardiosclerosis in patients with severe myocarditis. The absence of large-focal cardiosclerosis with correctly performed scintigraphy is an important argument against IHD. Myocarditis is characterized by a diffuse, uneven distribution of the radiopharmaceutical in the myocardium, which indicates a non-coronarogenic lesion; these changes are detected during examination at rest and can intensify with exercise, indicating inflammatory damage to the intramyocardial vessels (myocardial vasculitis). Detection focal changes perfusion also does not exclude myocarditis. A method has been proposed for myocardial tomoscintigraphy with autoleukocytes labeled with 99 Tc-HMPAO, which quite effectively identifies areas active inflammation, however, its implementation is quite labor-intensive.
MRI of the myocardium with gadolinium is considered as the most accurate method for non-invasive detection of foci of active inflammation in the myocardium (typically identifying zones of delayed accumulation of gadolinium); however, the absence of changes on MRI does not exclude the diagnosis of myocarditis. Indirect signs Myopericarditis is caused by thickening of the pericardial layers and the presence of a small amount of fluid in its cavity. MRI also allows for differential diagnosis with a number of heart diseases (complex malformations, MI, non-compact myocardium, amyloidosis, HCM, arrhythmogenic right ventricular dysplasia, etc.).
Similar changes can be detected during MSCT with intravenous contrast. This method also allows us to identify
calcium inclusions in constrictive pericarditis, intracardiac thrombosis and, very importantly, signs of atherosclerotic or inflammatory (as part of systemic vasculitis) damage to the coronary arteries and aorta.
In order to exclude coronary atherosclerosis as a cause of unexplained heart failure, pain in the heart area, and rhythm disturbances, in some cases (when non-invasive techniques do not provide sufficient information), coronary angiography is performed.
Finally, the gold standard for diagnosing myocarditis is endomyocardial biopsy. The diagnostic value of this method for myocarditis is very high (although very uncertain data can be obtained for focal myocarditis); its widespread use is limited by the invasive nature of the procedure, the unsafety of its implementation is not enough experienced specialists and the need for highly qualified and versatile morphological research of the obtained material.
Endomyocardial biopsy consists of inserting into the cavity of the right (through the subclavian or femoral vein), less often - the left ventricle (through the femoral artery) with a special instrument - a biotome - in order to obtain pieces of the endocardium and myocardium under the control of fluoroscopy, echocardiography or MRI. It is optimal to collect 5–6 pieces from different parts of the heart; carry out histological, electron microscopic, immunohistochemical and virological (using PCR diagnostics) analysis of the obtained material.
The Dallas criteria are used to make the diagnosis of myocarditis.
1. Active myocarditis:
infiltrate (diffuse or local);
quantitative counting using the immunohistochemical method (not less than
14 infiltrating lymphocytes per 1 mm2 (mainly CD45+ T lymphocytes or activated T lymphocytes) and up to 4 macrophages);
necrosis or degeneration of cardiomyocytes;
fibrosis (its development is not considered mandatory).
2. Borderline myocarditis:
infiltrate (at least 14 lymphocytes and up to 4 macrophages per 1 mm 2 );
necrosis and degeneration are usually not expressed;
fibrosis is taken into account.
3. Absence of myocarditis:
There are no infiltrating cells or their number does not exceed 14 per
1 mm2.
The study of biopsy specimens allows us to determine the genome of cardiotropic viruses, diagnose special forms of myocarditis (giant cell, eosinophilic, granulomatous, etc.), as well as carry out differential diagnosis with other non-coronary myocardial diseases and determine indications for specific treatment.
Diagnostics
To establish the diagnosis of severe acute myocarditis, the New York Classification of Chronic Heart Failure (NYHA) criteria are used.
1. The existence of an infection proven laboratory or clinically (including isolation of the pathogen, dynamics of titers of antimicrobial or antiviral antibodies, the presence of acute phase indicators - an increase in ESR, the appearance of CRP).
2. Signs of myocardial damage:
Big signs:
§ pathological changes on the ECG (impaired repolarization, rhythm and conduction);
§ increasing the concentration of cardioselective enzymes and proteins (CPK, MV-CPK, LDH, troponin T);
§ increase in heart size according to radiography or echocardiography;
§ cardiogenic shock;
Minor signs:
§ tachycardia (sometimes bradycardia);
§ weakening of the first tone;
§ gallop rhythm.
The diagnosis of myocarditis is valid when a previous infection is combined with one major and two minor signs.
According to the leading clinical symptom (syndrome) there are clinical options myocarditis:
1. decompensatory;
2. arrhythmic;
3. pseudocoronary;
4. pseudovalvular;
5. thromboembolic;
6. mixed;
7. low-symptomatic.
All of the listed symptoms of myocarditis can be expressed to varying degrees or completely absent, which gives grounds to distinguish mild, moderate and severe forms of the disease. Based on the results of long-term observation of patients with myocarditis, N. R. Paleev et al. The following are identified as the most typical
variants of the course of myocarditis:
1. Acute mild myocarditis.
2. Acute severe myocarditis.
3. Myocarditis (subacute) recurrent course.
4. Myocarditis (subacute) with increasing dilation of the cavities.
5. Chronic myocarditis.
There are special forms of myocarditis:
1. Eosinophilic (hypersensitivity, allergic)
myocarditis - often develops in response to exposure to an allergen (most often a drug), characterized by a high level of eosinophils in the blood, concomitant eosinophilic lesions of other organs (skin, lungs, blood vessels), detection of eosinophilic infiltrates in the myocardium and endocardium, pronounced positive effect glucocorticoid therapy. In addition, in a number of patients there is no pronounced blood eosinophilia, but the presence immune diseases other organs, high titers of anticardiac antibodies, an increase in nonspecific immune markers in the blood, combined with the absence of signs of viral infection, also create conditions for the effectiveness of glucocorticoid therapy.
2. giant cell- clinically differs from other forms in the extreme severity of the course; the diagnosis can only be made using endomyocardial biopsy and requires aggressive immunosuppressive therapy, which is not always effective. In some cases histological picture giant cell myocarditis is detected in Abramov-Fiedler myocarditis.
3. Abramov-Fiedler myocarditis - diagnosed clinically on the basis of an extremely severe course of the disease, which ends in death at a fairly early stage. Such severe damage to the heart with rapid (within 4 months) development of its dilatation and death was described in 1897 by S. S. Abramov (a morphological study of the myocardium revealed severe degeneration of cardiomyocytes and necrosis) and in 1899 by A. Fiedler ( who observed infiltrates in the myocardium and identified severe myocarditis as a separate form). The causes of the disease remain unknown, although direct viral damage to the myocardium in combination with an inadequate immune response has been suggested in predisposed, usually young, patients. The cause of death may be progressive heart failure, severe, life-threatening rhythm and conduction disorders, embolism different localization, the source of which is intracardiac (intertrabecular) thrombi. Death may occur suddenly.
Differential diagnosis
Depending on the course of myocarditis, differential diagnosis is carried out with various diseases.
1. For mild (latent, minimally manifest) myocarditis, which occurs without heart failure, differential diagnosis is carried out with NCD, so-called idiopathic or genetically determined disorders of cardiac rhythm and conduction (with various channelopathies, arrhythmogenic dysplasia of the right ventricle, etc.). The gradually progressive nature of arrhythmias, the addition of signs of heart failure in relatively young people require the exclusion of congenital myopathies and various genetically determined myocardial diseases, which cannot always be attributed to a specific type of cardiomyopathy (hypertrophic, restrictive, dilated).
2. Acute myopericarditis with intense pain in the heart, ST segment elevation and the appearance of a negative T wave on the ECG, an increase in blood troponin levels requires differential diagnosis with MI, stress-induced cardiomyopathy.
3. Pseudovalvular variant of myocarditis(with the development of valvulitis,
secondary valve dysfunction, usually of the type of insufficiency), as well as the development of acute myocarditis in combination with persistent fever;
after streptococcal infection may require differential diagnosis with rheumatic carditis, IE.
4. Severe myocarditis most difficult to differentiate from primary, genetically determined DCM. In this case, it is necessary to pay attention to a burdened family history, the age of onset of the disease and its connection with past infection, the severity of symptoms, the rate of progression, the presence of markers of viral infection and immune inflammation, information about the effectiveness of antiviral, antibacterial, and immunosuppressive therapy in the anamnesis. In some cases, assistance in diagnosing DCM can be provided by genetic research However, the most significant method for excluding active myocarditis is endomyocardial biopsy.
Formulation clinical diagnosis includes the following items:
1. etiological factor (if known);
2. clinical-pathogenetic variant (infectious, infectious-immune, toxic, etc.);
3. severity of the course (mild, moderate, severe);
4. nature of the course (acute, subacute, chronic);
5. the presence of complications: heart failure, thromboembolic syndrome, rhythm and conduction disturbances, relative insufficiency of the mitral and (or) tricuspid valve, etc.
Treatment of myocarditis, especially severe and moderate, as well as chronic, is a rather complex task due to insufficient knowledge of the etiology and mechanisms of development of the disease, the impossibility in many cases of endomyocardial biopsy, the severity of the disease, and the lack of large studies to study the effectiveness various types therapy.
In some cases, acute myocarditis ends with spontaneous recovery, but it is quite difficult to predict such an outcome.
When prescribing treatment for patients with myocarditis, take into account:
1. etiological factor;
2. pathogenetic mechanisms;
3. severity of myocardial damage syndrome (in particular, the presence of heart failure and rhythm and conduction disorders).
The impact on the etiological factor (if it is known) involves the following measures.
1. Patients with infectious and Infectious-toxic myocarditis (myocarditis that occurs during an infection or shortly after its disappearance) is usually prescribed antibiotics, most often benzylpenicillin at a dose of 1.5–2.0 million units/day or semisynthetic penicillins for 10–14 days. Suppression of focal infection (usually the upper respiratory tract, bronchopulmonary apparatus) promotes favorable outcome diseases.
2. In acute myocarditis of unknown etiology, occurring with fever and severe general inflammatory changes, combination therapy with broad-spectrum antibiotics is performed.
3. With an established viral etiology of myocarditis (including when a viral genome is detected in myocardial biopsies), etiotropic therapy depends on the type of virus: detection of entero- and adenoviruses implies the administration of interferon beta; herpes viruses type 1 and 2 – acyclovir; herpes virus type 6, cytomegalovirus, EpsteinBarr virus - ganciclovir, parvovirus B19 - intravenous administration of immunoglobulin in a total dose 0.2–2.0 g/kg body weight. Immunoglobulin can also be used in the treatment of other viral myocarditis, since it has both antiviral and immunomodulatory effects. In some cases, the effectiveness of antiviral therapy is not high enough, but attempts at its implementation are always justified. In chronic myocarditis, especially severe and moderate, elimination of the virus from the myocardium apparently leads to improvement functional state myocardium (reducing the size of the chambers, increasing myocardial contractility), and long-term persistence of the virus worsens the prognosis.
4. Treatment of the disease against which myocarditis developed (for example, SLE) is mandatory, since myocarditis is essentially component of this disease.
5. Elimination of the influence of various external pathogenic factors is also considered as the best means of preventing the disease and preventing its relapse in chronic cases.
Pathogenetic therapy involves the following measures.
1. Prescription of immunosuppressive and anti-inflammatory treatment. Unconditional indications for immunosuppressive treatment are eosinophilic (hypersensitivity), giant cell myocarditis, myocarditis in diffuse connective tissue diseases and systemic vasculitis, as well as myocarditis with pronounced (including systemic) immune disorders in the absence of markers of viral infection. It is assumed that the virus was not only not detected in the blood, but to exclude the persistence of the virus in the myocardium, an endomyocardial biopsy was performed, but in practice this is not always possible. To some extent, the participation of viruses in the development of the disease can be judged by the concentration of antiviral antibodies in the blood.
2. For severe and moderate myocarditis, prednisolone is prescribed at a dose of 1 mg/kg per day; At the same time, it is possible to prescribe azathioprine 2 mg/kg or cyclosporine 5 mg/kg. After a week, begin a gradual reduction in the dose of prednisolone to a maintenance dose (5 mg/day); the total duration of treatment is at least six months. A milder regimen of glucocorticoid therapy is also possible - prescribing prednisolone in the starting dose 30–40 mg/day with a gradual decrease after 1–2 months. At mild flow myocarditis, the starting dose of prednisolone can be 20 mg/day. In addition, they are used (as monotherapy for mild myocarditis or additionally
To glucocorticoids – for severe and moderate severe course) preparations of aminoquinoline derivatives – hydroxychloroquine and chloroquine (according to 1-2 tablets at a dose of 0.25 g or 0.2 g 1-2 times a day for 6 months or more.
2. In a situation where myocarditis occurs with severe immune disorders (in particular, the titer of anticardiac antibodies is significantly increased) and at the same time markers of a viral infection are detected, antiviral treatment may precede immunosuppressive therapy or (in severe acute myocarditis) it is carried out simultaneously.
3. To influence the nonspecific component of inflammation in acute myocarditis (or exacerbation of chronic) of any severity, NSAIDs are prescribed in standard doses. The most commonly used is indomethacin (0.025 g each 3–4 times a day), diclofenac (100–150 mg/day), as well as meloxicam (7.5–15 mg/day) or celecoxib (100–200 mg/day for 4–8 weeks) . For severe myocarditis, NSAIDs can be combined with prednisolone.
4. The effectiveness of drugs that affect individual links in pathogenesis (for example, a drug represented by monoclonal antibodies to TNF-a, - infliximab) in myocarditis has been practically not studied. The use of drugs that improve metabolic processes in the myocardium (trimetazidine at a dose of 75 mg/day, etc.) plays only a supporting role in the treatment complex.
5. Immunosorption is recommended as a method for effectively removing excess amounts of anticardiac antibodies.
The impact on myocardial damage syndrome involves the treatment of heart failure, rhythm and conduction disorders, as well as thromboembolic syndrome.
1. Treatment of patients withheart failure carried out according to generally accepted principles (bed rest, restriction table salt, ACE inhibitors, β-blockers, diuretics, and, if necessary, cardiac glycosides). The effect of cardiac glycosides in these cases is not as pronounced as in heart failure caused by hemodynamic overload of certain parts of the heart. In patients with myocarditis, phenomena of glycoside intoxication, ectopic arrhythmias, and conduction disturbances occur more quickly, and therefore you should be especially careful when prescribing these drugs. Diuretics are prescribed taking into account the stage of heart failure (for more information about the principles and tactics of treatment with cardiac glycosides and diuretics, see “Heart failure”).
2. Destination options antiarrhythmic drugs in severe myocarditis are also limited: the increased risk of developing a proarrhythmic effect makes the prescription of class I antiarrhythmics inappropriate and requires caution when prescribing amiodarone. At the same time, amiodarone and calcium antagonists, as well as β-blockers, can significantly reduce cardiac output in patients with initially low ejection fraction. Ivabradine can be successfully used to reduce the severity of sinus tachycardia, which develops in heart failure. 10–15 mg/day.
3. Thromboembolic syndromerecorded in patients with severe myocarditis (most often with myocarditis of the Abramov-Fiedler type). Indications of a history of thromboembolism and intracardiac thrombosis (proven by echocardiography, MRI or MSCT

heart) - indications for the use of indirect anticoagulants (especially with low left ventricular ejection fraction). The detection of severe heart failure and AF (of any form) in patients with myocarditis, as a rule, also serves as an indication for their use.
With severe and especially fulminant myocarditis, there may be a need for active inotropic support of the myocardium (intravenous administration of dobutamine, dopamine, levosimendan), artificial replacement of the function of vital organs - artificial ventilation, ultrafiltration, hemodialysis, as well as temporary use of circulatory support systems. The patient’s life often depends on the timeliness of these measures.
Possibilities surgical treatment myocarditis are limited, which follows from the characteristics of the disease itself (an active inflammatory process, usually diffusely affecting the heart muscle). Surgical intervention may be aimed at eliminating the irreversible consequences of myocarditis (implantation of a permanent pacemaker, cardiac resynchronization device, ICD, heart valve replacement, in some cases - reconstructive operations on the heart). A radical method of surgical treatment of extremely severe myocarditis, which is used in cases of complete ineffectiveness of drug therapy and auxiliary surgical techniques, heart transplantation is used (if the virus persists in the myocardium, a complete anatomical heart transplant is preferable). However, relapse of the disease in the transplanted heart cannot be ruled out.
For mild and moderate myocarditis, the prognosis is usually favorable. It is much more serious with severe myocarditis, and unfavorable with myocarditis of the Abramov-Fiedler type.
Myocarditis: signs, causes, diagnosis, therapy
Myocarditis is a cardiac disease, namely inflammation of the heart muscle (myocardium). The first studies on myocarditis were carried out in the 20-30s of the 19th century, therefore modern cardiology has a wealth of experience in the diagnosis and treatment of this disease.
Myocarditis is not “tied” to a certain age, it is diagnosed in both older people and children, and yet it is most often observed in 30-40 year olds: less often in men, more often in women.
Types, causes and symptoms of myocarditis
There are several classifications of myocarditis - based on the degree of damage to the heart muscle, the form of the disease, etiology, etc. Therefore, the symptoms of myocarditis also vary: from a latent, almost asymptomatic course - to the development of severe complications and even sudden death patient. Pathognomonic symptoms of myocarditis, that is, those that unambiguously describe the disease, unfortunately, are absent.
The main, universal signs of myocarditis include a general loss of strength, low-grade fever, rapid fatigue during physical activity, accompanied by disturbances in the heart rhythm, shortness of breath and palpitations, and increased sweating. The patient may experience some discomfort in the chest on the left and in the precordial area and even prolonged or constant painful sensations pressing or stabbing nature (cardialgia), the intensity of which does not depend on the size of the load or the time of day. Volatile pain in the muscles and joints (arthralgia) may also be observed.
Myocarditis in children is diagnosed as a congenital or acquired disease. The latter most often becomes a consequence of ARVI. In this case, the symptoms of myocarditis are similar to the symptoms of the disease in an adult: weakness and shortness of breath, lack of appetite, restless sleep, manifestations of cyanosis, nausea, vomiting. The acute course leads to an increase in the size of the heart and to the formation of the so-called cardiac hump, rapid breathing, fainting, etc.
Among the forms of the disease, acute myocarditis and chronic myocarditis are distinguished. Sometimes we are also talking about a subacute form of myocardial inflammation. Various degrees localization/prevalence of the inflammatory process in the heart muscle also allows us to distinguish diffuse myocarditis and focal ones, and various etiologies serves as a basis for highlighting the following groups and types of myocardial inflammation.
Infectious myocarditis
The second place is occupied by bacterial myocarditis. Thus, the cause of rheumatic myocarditis is, and the main causative agent of the disease is beta-hemolytic streptococcus of group A. Among the main symptoms of this type of myocarditis are palpitations and shortness of breath, increasing chest pain, and in severe cases of the disease, also acute left ventricular failure in the form of or alveolar pulmonary edema, accompanied by moist rales in the lungs. Over time, it may develop with the appearance of edema, involvement of the liver, kidneys, and accumulation of fluid in the cavities.
The cause of myocarditis in parallel can be two or more infectious pathogens: one creates favorable conditions for this, the second directly “deals” with damage to the heart muscle. And all this is often accompanied by an absolutely asymptomatic course.
Myocarditis of non-rheumatic origin
Myocarditis of non-rheumatic origin manifests itself predominantly in the form of allergic or infectious-allergic myocarditis, which develops as a consequence of an immunoallergic reaction.
Allergic myocarditis is divided into infectious-allergic, medicinal, serum, post-vaccination, burn, transplantation, or nutritional. It is most often caused by a reaction of the human immune system to vaccines and serums that contain proteins from other organisms. Pharmacological drugs that can provoke allergic myocarditis include some antibiotics, sulfonamides, penicillins, catecholamines, as well as amphetamine, methyldopa, novocaine, spironolactone, etc.
Toxic myocarditis It can be a consequence of a toxic effect on the myocardium - with alcoholism, hyperfunction of the thyroid gland (hyperthyroidism), uremia, poisoning with toxic chemical elements, etc. Insect bites can also provoke inflammation of the myocardium.
Symptoms of allergic myocarditis include heart pain, general malaise, palpitations and shortness of breath, possible joint pain, and elevated (37-39°C) or normal temperature. Intracardiac conduction disturbances and heart rate: tachycardia, bradycardia (less often), .
The disease begins asymptomatically or with minor manifestations. The severity of the signs of the disease is largely determined by the localization and intensity of the development of the inflammatory process.
Abramov-Fiedler myocarditis
Abramov-Fiedler myocarditis (another name is idiopathic, which means it has an unclear etiology) is characterized by a more severe course, accompanied, that is, by a significant increase in the size of the heart (the reason for which is pronounced), serious disturbances in cardiac conduction and rhythm, which ultimately results in heart failure.
This type of myocarditis is observed more often in middle age. Often it can even lead to death.
Diagnosis of myocarditis
Making a diagnosis such as “myocarditis” is usually complicated by the latent course of the disease and the ambiguity of its symptoms. It is carried out on the basis of a survey and anamnesis, physical examination, laboratory blood test and cardiographic studies:
Physical examination of myocarditis reveals an enlargement of the heart (from a slight displacement of its left border to a significant increase), as well as congestion in the lungs. The doctor notes that the patient has swelling of the neck veins and swelling of the legs, cyanosis is likely, that is, blueness of the mucous membranes, skin, lips and tip of the nose.

Upon auscultation, the doctor detects moderate or symptoms of left and right ventricular failure, a weakening of the first tone and a gallop rhythm, and listens to a systolic murmur at the apex.
- A laboratory blood test is also informative in diagnosing myocardial inflammation. General blood analysis may show a shift to the left in the leukocyte formula, an increase, an increase in the number ().
demonstrate dysproteinemia (deviations in the quantitative ratio of blood protein fractions) with hypergammaglobulinemia ( increased level immunoglobulins), the presence of increased content seromucoid, sialic acids, fibrinogen.
Blood culture able to attest to the bacterial origin of the disease. During the analysis, the antibody titer indicator is also determined, informing about their activity.
- Radiography chest shows expansion of the boundaries of the heart, and sometimes congestion in the lungs.
- , or ECG, is a diagnostic technique for studying the electric fields generated during the work of the heart. When diagnosing myocarditis, this research method is very informative, since changes in the electrocardiogram in case of disease are always noted, although they are not specific. They appear as nonspecific transient changes in the T wave (flattening or decreasing amplitude) and ST segment (displacement up or down from the isoelectric line). Pathological Q waves and a reduction in the amplitude of R waves in the right precordial leads (V1-V4) can also be recorded.
Often the ECG also shows ventricular and supraventricular extrasystole. An unfavorable prognosis is indicated by episodes and, which indicates extensive inflammatory foci in the myocardium.
- – an ultrasound method that examines morphological and functional abnormalities in the activity of the heart and its valves. Unfortunately, it is not possible to talk about specific signs of myocardial inflammation during echocardiography.
When diagnosing myocarditis, echocardiography can detect various disorders of the myocardium associated with its contractile function (primary or significant dilatation of the cardiac cavities, decreased contractile function, diastolic dysfunction, etc.), depending on the severity of the process, as well as identify intracavitary thrombi. It is also possible to detect an increased amount of fluid in the pericardial cavity. At the same time, cardiac contractility indicators during echocardiography may remain normal, which is why echocardiography has to be repeated several times.
Auxiliary methods for diagnosing myocarditis, allowing you to prove the correctness of the diagnosis, can also be the following:
- Isotope study of the heart.
- Endomyocardial biopsy and others.
The latter method is today considered by many doctors to be sufficient for precise setting diagnosis of “myocarditis”, however, this situation still raises some doubts, since endomyocardial biopsy can give many ambiguous results.
Treatment of myocarditis
Treatment of myocarditis includes etiotropic therapy and treatment of complications. The main recommendations for patients with myocarditis will be hospitalization, providing rest and bed rest (from 1 week to 1.5 months - according to the severity), the prescription of oxygen inhalations, as well as the use of non-steroidal anti-inflammatory drugs (NSAIDs).
Diet during the treatment of myocarditis involves limited consumption salts and liquids when the patient exhibits signs of circulatory failure. A etiotropic therapy is the central link in the treatment of myocarditis– focused on eliminating the factors that caused the disease.
Treatment of viral myocarditis directly depends on its phase: Phase I – the period of pathogen reproduction; II – stage autoimmune damage; III – dilatation, or DCM, that is, stretching of the cardiac cavities, accompanied by the development of systolic dysfunction.
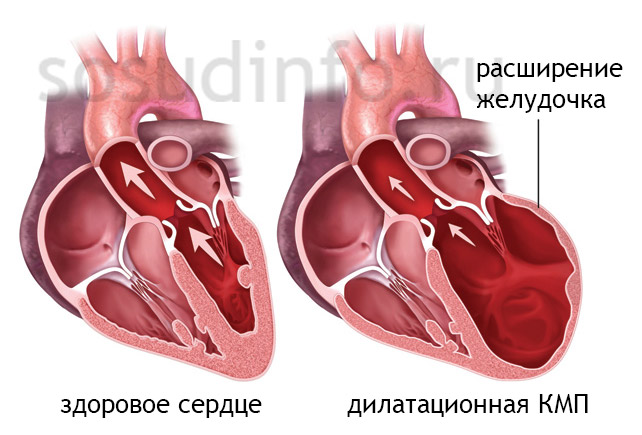
a consequence of the unfavorable course of myocarditis – dilated cardiomyopathy
The prescription of drugs for the treatment of viral myocarditis depends on the specific pathogen. Patients are indicated for maintenance therapy, immunization, reduction or complete elimination of physical activity until the symptoms of the disease disappear, functional indicators stabilize and the natural, normal size of the heart is restored, since physical activity promotes the resumption (replication) of the virus and thereby complicates the course of myocarditis.

The cardinal measure in the treatment of myocarditis is transplantation, i.e.: it is performed on the condition that the therapeutic measures taken did not improve functional and clinical indicators.
Prognosis for myocarditis
The prognosis for myocarditis, unfortunately, is very variable: from full recovery to death. On the one hand, myocarditis often progresses latently and ends with absolute recovery. On the other hand, the disease can lead, for example, to, accompanied by the growth of connective scar tissue in the myocardium, deformation of the valves and replacement of myocardial fibers, which then leads to persistent disturbances in heart rhythm and its conductivity. To the number likely consequences Myocarditis also refers to a chronic form of heart failure, which can cause disability and even death.
Therefore, after hospitalization, a patient with myocarditis is under clinical observation for another year. He was also recommended for sanatorium treatment in cardiological institutions.
Outpatient observation is mandatory, which involves examination by a doctor 4 times a year, laboratory tests of blood (including biochemical analysis) and urine, as well as ultrasound of the heart - once every six months, and a monthly ECG. Regular immunological studies and testing for viral infections are also recommended.
Measures to prevent acute myocarditis are determined by the underlying disease that caused this inflammation, and are also associated with particularly careful use of foreign serums and other drugs that can cause allergic and autoimmune reactions.
And one last thing. Considering how serious the complications of myocarditis can be, it is extremely imprudent to self-medicate inflammation of the heart muscle using “grandmother’s methods”, various folk remedies or medications without a doctor’s prescription, as it can lead to serious consequences. And vice versa: timely detection of myocarditis symptoms and appropriate comprehensive treatment in the cardiology department of a medical institution always has a positive effect on the prognosis of patients.
Video: myocarditis in the program “Live Healthy!”
On the topic of: Non-rheumatic myocarditis
Performed by an intern
Ostankova A. Yu.
Semipalatinsk
Non-rheumatic myocarditis (NM) is an inflammatory disease of the myocardium caused by infectious, allergic, toxic effects with various pathogenetic mechanisms.
Classification
| Etiology |
Pathological data |
Severity |
Circulatory failure |
Inflammatory lesions of the myocardium constitute a large group of diseases, the study of which until recently has been insufficient. This is due to the fact that the main attention was aimed at combating rheumatism, although in a significant group of patients myocarditis develops without connection with the rheumatic process. As pathological studies have shown, the prevalence of urinary incontinence among children is higher (6.8%) than among adults (4%). Etiology. See classification. Sometimes the etiology may not be established, in such cases they speak of idiopathic myocarditis. Pathogenesis is different, which is associated with a variety of etiological factors. However, most UI does not arise as a result of direct exposure to infection, but in connection with a certain state of sensitization of the child’s body to various agents - bacterial, chemical, physical. Such myocarditis can be combined under the concept of infectious-allergic. When they occur, immune complexes are fixed in the walls of blood vessels, and therefore cell membranes are damaged with the activation of hydrolytic enzymes of lysosomes. All this leads to denaturation of proteins and their acquisition of autoantigenic properties. In the pathogenesis of some myocarditis, purely allergic mechanisms play a role (with serum sickness, reactions to medications, vaccinations). During Coxsackie infection, the invasion of this virus into the myocardial cell, leading to its destruction and the release of lysosomal enzymes, is of key importance. At the same time, with influenza, the role of immunological mechanisms is more significant. However, not all children who have had infectious diseases suffer from UI. The state of reactivity of the macroorganism plays a major role in the development of the disease. At an early age, the child’s reactivity can be influenced by toxicosis of pregnancy suffered by the mother, acute and chronic illnesses, previous abortions and miscarriages, as well as various perinatal infections and constitutional anomalies in the child. Children from the group of frequently and long-term ill patients are also susceptible to UI. Age aspect. NM occurs in all age groups. Family aspect. The factor that plays a role in the occurrence of urinary incontinence in children is hereditary predisposition. It has been established that close relatives of a sick child have frequent cases of pathology of the cardiovascular system and allergic diseases. Children brought up surrounded by carriers of chronic foci of infection (parents and other relatives) are more likely to get sick. Diagnostic criteria In practice, they use the criteria proposed by the New York Heart Association (1964, 1973) as modified by Yu.I. Novikova et al. (1979). Supporting features: previous infection, proven clinically and laboratory methods, including isolation of the pathogen, results of the neutralization reaction (RN), complement fixation (RSK), hemagglutination (RHA); · signs of myocardial damage (increase in heart size, weakening of 1 tone, cardiac arrhythmia, systolic murmur); presence of persistent pain in the heart area, often unrelieved vasodilators; · pathological changes on the ECG, reflecting disturbances in excitability, conductivity, and automaticity of the heart, characterized by resistance, and often refractoriness to targeted therapy; · early appearance signs of left ventricular failure followed by the addition of right ventricular failure and the development of total heart failure; · increased activity of serum enzymes (CPK, LDH); · changes in the heart with ultrasound echocardiography: enlargement of the left ventricular cavity; hypertrophy of the posterior wall of the left ventricle; hyperkinesia interventricular septum; decline contractility left ventricular myocardium. Optional signs: · burdened heredity; · previous allergic mood; general weakness: · temperature reaction; · changes in blood tests characterizing the activity of the inflammatory process. Laboratory and instrumental research methods Basic methods: Complete blood count (moderate leukocytosis, increased ESR); · general urine analysis (normal), with congestion – proteinuria; · biochemical blood test: increased levels of DPA, CRP, enzyme activity (LDG, CPK); · laboratory tests to identify the pathogen: RN, RSK, RGA; · ECG (decrease in wave voltage, rhythm disturbance, change in S-T interval, etc.); · radiography of the heart (determining the size of the heart). Additional methods: · level determination total protein and its fractions in blood serum; · Ultrasound of the heart; · immunological studies (determination of the content of immunoglobulins, T- and B-lymphocytes, complement); · polycardiography (polyCG). Examination stages In the office family doctor: taking anamnesis (previous infectious or allergic diseases, hereditary history); objective examination (pulse pattern, blood pressure, presence of arrhythmia, changes in the boundaries of the heart, liver size, presence of edema). At the clinic: general blood and urine tests, biochemical blood tests, chest x-ray, consultation with a cardiologist. In the clinic: determination of enzyme levels, RSC, RGA, polyCG, ultrasound of the heart. All blood tests are done on an empty stomach. Course, complications, prognosis Clinical course options In severe forms of carditis, signs of intoxication are observed, and the child’s general condition suffers significantly. Body temperature can rise to 39°C. Signs of circulatory failure appear early. By percussion and x-ray, the expansion of the borders of the heart is determined. In some children, a rough systolic murmur is heard over the apex of the heart, which indicates relative insufficiency of the bicuspid valve. If such a noise persists for a long time during treatment and with a decrease in the size of the heart, this indicates damage to the valve apparatus (sclerosis of the papillary muscles and chords), hemodynamic or organic deformation of the valve leaflets. In the case of pericarditis, tachycardia, dullness of heart sounds increase, and a pericardial friction noise is heard. Severe forms of UI include diseases that occur with complex disturbances in the rhythm and conduction of the heart. This form of UI is more common in young children (with congenital and acquired carditis). The moderate form of UI can occur in both young and older children and is characterized by low-grade fever body for 1-2 weeks, pale skin, fatigue. The degree of intoxication is less pronounced. All the symptoms of carditis are present. Signs of circulatory disorders correspond to Art. II A. The mild form occurs in older children and is extremely rare in early childhood. It is characterized by a paucity of signs of the disease. General state in such children there is little impairment. The borders of the heart are normal or expanded to the left by 0.5-1 cm. There is a slight tachycardia, more pronounced in young children with rhythm disturbances. Clinical signs of circulatory failure correspond to stage I. or missing. There are changes in the ECG. A feature of UI in children is the variety of types of their course, which can be acute, subacute, chronic (see classification). At acute course the onset of myocarditis is rapid, a clear connection is established between its development and an intercurrent disease, or it occurs soon after a preventive vaccination. The leading place at the onset of the disease is occupied by non-cardiac symptoms: pallor, irritability, poor appetite, vomiting, abdominal pain, etc. And only after 2-3 days, and sometimes later, signs of heart damage appear. In young children, the onset of the disease may be attacks of cyanosis, shortness of breath, and collapse. The subacute type of urinary incontinence develops gradually and is accompanied by moderately severe clinical symptoms. The disease manifests itself by asthenia 3-4 days after a viral or bacterial infection. Initially, general signs of the disease appear: irritability, fatigue, poor appetite, etc. Body temperature may be normal. Cardiac symptoms develop gradually and in some children they appear against the background of repeated ARVI or preventive vaccination. The chronic course of UI is more common in older children and occurs as a consequence of acutely or subacutely onset myocarditis or in the form of a primary chronic form that develops gradually with an asymptomatic initial phase. In young children, carditis developed in utero may have a chronic course. |
Myocarditis– a disease characterized by the development of an inflammatory process in the myocardium (heart muscle). It may be caused by infection, allergic reactions, or toxic effects. All myocarditis can be divided into two large groups: rheumatic and non-rheumatic. Non-rheumatic myocarditis most often affects young people, usually women. The prevalence of the disease is 5-10% of all pathologies of the cardiovascular system.
Non-rheumatic myocarditis often occurs in mild form and passes quickly, so it is very difficult to calculate exact incidence rates.
Anatomical features of the structure of the heart
Heart – muscular organ, located in chest. Its function is to ensure the movement of blood through the vessels.Layers of the heart wall:
- Endocardium- inner layer. Lines the inside of all the chambers of the heart.
- Myocardium– the thickest, muscular layer. It is most developed in the area of the left ventricle, least of all in the area of the atria.
- Epicard- the outer lining of the heart, which performs protective functions and secretes a lubricant that reduces friction during contractions.
Types of myocardiocytes(muscle cells in the heart wall):

- Typical contractile muscle cells. They provide the main function of contracting and pushing blood.
- Atypical myocytes– transformed muscle cells, playing the role of a kind of autonomous nervous system organ. They conduct electrical impulses, causing typical myocardiocytes to contract.
Chambers of the heart:

- Right and left atria. Receive venous blood from the superior and inferior vena cava, respectively (flows from organs and tissues), arterial blood from the pulmonary veins (returns to the heart from the lungs, being enriched with oxygen). They do not bear high loads, so their muscle layer is thin.
- Right ventricle. Receives venous blood from the right atrium and pushes it into the lungs, into the pulmonary circulation, where it is enriched with oxygen.
- Left ventricle. Receives arterial blood from the left atrium and pushes it into the systemic circulation, to all organs and tissues. It does the most intense work, so its muscle wall is the thickest.
- An electrical impulse occurs in the upper part of the interatrial septum, in a collection of atypical myocytes called the sinus node (or pacemaker).
- The electrical impulse from the pacemaker spreads to the walls of the atria. Their systole (contraction) occurs. Blood from the atria is pushed into the ventricles.
- The electrical impulse propagates to the wall of the ventricles. They contract, pushing blood into the systemic and pulmonary circulation. At this time, diastole (relaxation) of the atria occurs.
- Diastole of the atria and ventricles, after which a new impulse arises in the pacemaker.
- Direct damage to muscle fibers by infection and toxins.
- As a result of damage, some molecules that make up the myocardium are “exposed.” The immune system mistakes them for antigens (foreign bodies), and an allergic reaction develops, leading to even greater damage.
- Over time, muscle cells damaged as a result of inflammation are resorbed. In their place, areas of sclerosis form - microscopic scars.
What is diffuse myocarditis?
 With myocarditis, inflammation may involve different areas heart muscle. Depending on this, there are two types of myocarditis:
With myocarditis, inflammation may involve different areas heart muscle. Depending on this, there are two types of myocarditis: - Diffuse– the inflammatory process affects the entire heart muscle.
- Focal– inflammation is localized in one place, other areas of the myocardium remain unaffected.
Causes of myocarditis development
Classification of myocarditis depending on its origin:- Coxsackie A virus– the most common pathogen;
- adenovirus– just like the influenza virus, it is the causative agent of acute respiratory diseases;
- rubella virus.
What is acute and chronic myocarditis?
Types of myocarditis depending on the severity of the process:- Acute myocarditis. Starts off quickly. All symptoms of the disease appear very clearly. Body temperature usually rises greatly. All symptoms in the analyzes are clearly expressed.
- Subacute myocarditis. It starts more gradually. Lasts for a longer period of time. Changes in the analyzes are less pronounced.
- Chronic myocarditis. It lasts a long time. Periods of exacerbation alternate with periods of improvement.
Signs of myocarditis
Most often, myocarditis manifests itself with nonspecific symptoms, which also occur in many other diseases. There are no characteristic signs that would be detected exclusively in myocarditis.| Symptom | Short description |
| Pain |
|
| Feeling of interruptions in the work of the heart, increased and rapid heartbeat, a feeling as if the heart is “turning over”. | These symptoms can occur with a huge number of different states. They do not directly indicate myocarditis, but only make it clear that in this case the heart is “interested”. |
| Symptoms of heart failure |
|
| Weakness, slight increase in temperature, increased fatigue | They are detected in many patients, but are often caused not by myocarditis itself, but by the disease that served as the root cause (for example, infection). |
| Symptoms of the underlying disease that caused myocarditis |
|
Diagnosis of myocarditis
What does the doctor find during the examination?
| Symptom | Explanation |
| Visual inspection | |
| Signs of heart failure |
  |
| Percussion (tapping) | |
| The boundaries of the heart are expanded | The heart is enlarged because the muscle layer of its wall is thickened due to inflammation. The degree of heart enlargement is proportional to the severity of the disease. |
| Auscultation (listening with a phonendoscope) | |
| Muffled tones (sounds resulting from contractions) of the heart |  Due to the inflammatory process, the force of myocardial contraction is impaired. Due to the inflammatory process, the force of myocardial contraction is impaired. |
| Murmur at the apex of the heart | Most often it occurs due to extrasystoles - extraordinary contractions of the ventricles caused by irritation as a result of the inflammatory process. |
After examination by a doctor, in most cases it is still impossible to make an accurate diagnosis. The patient is scheduled for examination.
What tests detect myocarditis?
| Diagnostic method | Changes that can be detected | Explanation |
| ECG (electrocardiography)- a study in which electrical impulses arising in the heart are recorded in the form of a curve. Helps evaluate heart rhythm disturbances and myocardial condition. | ECG is normal. No changes were detected. | If no changes are detected on the electrocardiogram during myocarditis, then it can be very difficult to make a diagnosis. |
| These signs make it possible to more confidently make a diagnosis of myocarditis. | |
With myocarditis, changes on the ECG are inconsistent. They disappear on their own or after taking certain medicines. Special tests are based on this: an ECG is taken from the patient twice, before and after taking the medicine, and then the results are compared.  If changes in the ECG are persistent and do not disappear over time, then this may be due to chronic myocarditis, in which sclerosis occurs (development of scar tissue at the site of inflammation). If changes in the ECG are persistent and do not disappear over time, then this may be due to chronic myocarditis, in which sclerosis occurs (development of scar tissue at the site of inflammation). According to electrocardiography, myocarditis is often impossible to distinguish from coronary heart disease, hypertension, birth defects. The doctor makes a diagnosis after a comprehensive examination of the patient and full complex diagnostics |
||
| X-ray, computed tomography, magnetic resonance imaging. They allow you to visualize the heart, assess the degree of its enlargement and thickening of the walls. Ventriculography– a special study in which the chambers of the heart are pre-filled contrast agent, after which photographs are taken. | The size of the heart is not changed. | Myocarditis cannot be excluded, but diagnosis becomes problematic. |
| Only the left ventricle is enlarged. | The disease is most likely medium degree gravity. | |
| Severe myocarditis. | |
| Ultrasound of the heart– allows you to visualize the organ, assess the degree of its enlargement and the degree of thickening of the myocardium. |
| The severity of the changes indicates the severity of the inflammatory process. Ultrasound helps distinguish myocarditis from other diseases, such as valve defects.  |
| Doppler ultrasound and duplex scanning. These ultrasound techniques help assess blood flow in coronary vessels and cavities of the heart. | Mainly intended to distinguish myocarditis from other heart diseases. | |
| General blood analysis. |
| |
| Blood chemistry | Lineup changes:
| These changes indicate the presence of an inflammatory process in the body, a recent infection that could cause myocarditis. |
| Increased levels of certain enzymes: creatine phosphokinase, lactate dehydrogenase. | Indicates the destruction of muscle fibers in the heart as a result of inflammation. | |
| Testing the level of antibodies in the blood ( immunoglobulins). | An increase in the number of antibodies that protect the body from certain types of bacteria and viruses. | Current or past infection that may be causing myocarditis. |
| Immunological blood tests. | Changes indicating autoimmune reactions are detected. | Help confirm the allergic origin of myocarditis. |
It is often difficult to distinguish the different forms of myocarditis from each other. When making a diagnosis, the doctor must rely on all the data that he receives during the examination and questioning of the patient, and conducting an examination.
Signs of certain types of myocarditis
| Type of myocarditis | Signs |
| Infectious |
|
| Allergic |
|
| Idiopathic | No signs of any other diseases that can lead to myocarditis. |
| Burn | Suffered a severe burn. |
| Transplantation | Recent organ transplant. |
Features of rheumatic myocarditis
The symptoms of rheumatic myocarditis and the signs that a doctor identifies during examination are similar to those of non-rheumatic myocarditis. The same examination is carried out.Criteria for making a diagnosis of rheumatic myocarditis:
| Basic (“big”) criteria | Additional (“minor”) criteria |
Carditis(inflammatory heart disease):
| Previously diagnosed rheumatism, rheumatic lesion hearts. |
| Polyarthritis– inflammatory lesions of various joints. | Joint pain. |
| Chorea- damage to the nervous system. | Fever, increased body temperature for no apparent reason. |
| Ring-shaped erythema– skin lesions in the form of red rings. | An increase in the number of leukocytes and acceleration of erythrocyte sedimentation in a general blood test. |
| Nodules under the skin– rheumatic nodules. | Changes in the electrocardiogram. |
| Detection of increased amounts of C-reactive protein in biochemical analysis blood. |
Treatment of myocarditis
| A drug | Description | Directions for use and dosage |
| Antibiotics. They are used for infectious, infectious-toxic, infectious-allergic myocarditis, when a certain type of bacteria has been identified. Antibiotics are selected after bacteriological examination, depending on the sensitivity of the pathogen to them. |
||
| Erythromycin (syn.: Ilozon, Gryunamycin, Eomitsin, Sinerit, Eriderm, Erigeksal, Eritran, Eric, Erifluid, Erythroped, Ermitsed). | Erythromycin is an antibiotic effective against various types of bacteria. If used incorrectly and for too long, pathogens quickly develop resistance to it. | Release forms:
|
| Doxycycline (syn.: Vibramycin, Bassado, Apo-doxy, Doxidar, Doxibene, Doxal, Doxylin, Novo-Doxylin, Monoclin, Medomycin, Tetradox, Unidox, Etidoksin). | Antibiotic from the tetracycline group. Effective against almost all types of pathogenic bacteria. Compared to Tetracycline, it penetrates faster into organs and tissues after administration and is safer. | Release forms:
Adults: Children: |
| Monocycline | Antibacterial drug from the group of tetracyclines. Prevents the growth of bacteria. Acts on a large number of types of pathogenic microorganisms. | Release forms:
Adults:
|
| Oxacillin (syn.: Bristopen, Prostaflin). | Oxacillin is a synthetic drug from the penicillin group. Acts on a wide range of microorganisms, especially staphylococci. | Release forms:
|
| Antiviral drugs. With myocarditis of viral origin, antiviral drugs have little effectiveness. But they help cope with the underlying disease. |
||
| Interferon (syn.: Viferon, Grippferon) | Interferon is a substance that is produced in the human body and is a protective factor against various viruses. Human leukocyte interferon is used as a medicine. It is most effective as a means of prevention. During illnesses, its effectiveness is higher, the earlier it was prescribed. | Release forms:
Powder:
Insert the candle into anus 1 time per day in the appropriate dosage. |
| Ribavirin (syn.: Rebetol, Virazol, Ribamidil). | Ribavirin inhibits the synthesis of viral RNA and DNA molecules, thereby preventing the proliferation of viruses. It has no effect on human cells. The drug is effective against viruses that cause influenza, hepatitis, and herpes. | The drug is available in tablets of 0.2 g. Methods of application:
|
| Drugs that suppress immune responses. Their use is indicated for almost any form of myocarditis, since it has been proven that all of them are, to one degree or another, accompanied by autoimmune reactions. |
||
| Prednisolone (syn.: Prednihexal, Medopred, Decortin, Prednisol, Sherizolon). | Prednisolone is a hormone of the adrenal cortex. Has the ability to suppress immune reactions. Indications for use:
| For myocarditis, prednisolone is used in doses of 15–30 mg/day. The course of treatment lasts 2–5 days. For severe forms of disease, prednisolone is used in dosages of 60–80 mg/day. |
| Indomethacin (syn.: Indovis, Indobene, Apo- Indomethacin, Indopan, Indomin, Indofarm, Indotrad, Inteban, Indocid, Novo-Metacin, Methindol, Elmetacin, Tridocin). | Indomethacin is a drug belonging to the group of non-steroidal anti-inflammatory drugs. It is used to combat inflammatory and autoimmune processes in various diseases, including rheumatism. | Release forms:
In tablets:
Indomethacin is administered intramuscularly at a dosage of 0.06 g 1–2 times a day. The course of treatment lasts an average of 7 days. |
| Ibuprofen (syn.: Bolinetlingval, Advil, Bren, Bronifen, Burana, Brufen, DeepRilif, Children's Motrin, Ibusan, Ibupron, Dolgit, Ibuton, Ibutad, Nurofen, Motrin, Iprene, Profinal, Profen, Solpaflex, Reumafen). | A drug belonging to the group of non-steroidal anti-inflammatory drugs. One of the most modern and effective means. Suppresses education chemical substances, playing a role in inflammatory reactions. In addition to anti-inflammatory, it has antipyretic and analgesic effects. | Release forms:
Adults take ibuprofen in a dose of 0.2-0.8 g, 3-4 times daily. |
| Voltaren (syn.: Diclofenac, Ortofen, Diklo, Diclobene, Clofenac, Ecofenac, Etifenac, Diclonate, Sodium Diclofenac). | Belongs to the group of non-steroidal anti-inflammatory drugs. | Release forms:
In tablets:
By injection: Administer 0.075 g (1 ampoule) 1 – 2 times a day for 2 – 5 days. |
| Drugs that improve nutrition and metabolism in the heart muscle. Contributes to faster and full recovery myocardium. |
||
| Riboxin (syn.: Inosine, Inosie-F, Ribonosine) | Riboxin is converted in the body into ATP molecules - most important source energy for muscle cells. As a result of the use of this drug, the energy balance in the heart muscle increases. | Release forms:
|
| Potassium orotate | It is considered as an anabolic agent, as it enhances protein synthesis in myocardial cells. | Release forms:
Take one tablet 3 times daily, 1 hour before meals or 4 hours after meals. The course of treatment lasts 20–40 days. |
Additional treatment for the development of complications of myocarditis:
- For heart failure are appointed antihypertensive(reducing the level blood pressure) drugs, diuretics, drugs that stimulate the heart ( cardiac glycosides).
- For arrhythmias appropriate antiarrhythmic drugs. In case of severe heart damage, if necessary, the patient is given a pacemaker.
- For thrombosis as a result of circulatory disorders are prescribed anticoagulants(drugs that reduce blood clotting), fibrinolytics(drugs that dissolve blood clots).
Principles of treatment of rheumatic myocarditis
 Treatment of rheumatic myocarditis is carried out in accordance with the general principles of treatment of rheumatism:
Treatment of rheumatic myocarditis is carried out in accordance with the general principles of treatment of rheumatism: - Antibacterial therapy, aimed at combating the causative agent of the disease - streptococcus. Penicillin, oxacillin, ampicillin are used.
- To eliminate the inflammatory process applies Diclofenac And Indomethacin(see table above). Sometimes Aspirin is prescribed. These drugs are taken until all symptoms of the disease disappear completely.
- Suppression of autoimmune reactions with the help of Prednisolone and other drugs of adrenal cortex hormones is prescribed for severe cases of the disease.
How is myocarditis treated in children?
 Treatment of myocarditis in childhood is carried out according to the same principles as in adults (table above). All medications must be prescribed in age-appropriate dosages. Some of them are contraindicated for children.
Treatment of myocarditis in childhood is carried out according to the same principles as in adults (table above). All medications must be prescribed in age-appropriate dosages. Some of them are contraindicated for children. Prevention of myocarditis
There are no specific measures aimed at preventing myocarditis.General preventive measures:
- improving the overall standard of living of children;
- healthy lifestyle;
- hardening, healthy eating, taking vitamins;
- improvement of living conditions;
- combating overcrowding and timely isolation of patients from kindergartens, schools, and work groups;
- timely and full treatment any infections;
- reasonable prescription of antibiotics and other medications, their correct administration.
Forecast
The prognosis is favorable if myocarditis occurs in mild or moderate form. With severe myocarditis, the prognosis is more serious.Myocarditis is inflammation of the myocardium (heart muscle). The disease is common among children of various ages, but more often in 4–5 year olds and adolescents. The disease can occur in a latent form and is completely asymptomatic. Often it is recognized only after pronounced changes that are detected on the ECG.
Exists the following types diseases that differ in symptoms and processes occurring in the body:
- Infectious myocarditis– is directly related to infection of the body, appears against the background of illness or immediately after it. The infectious form begins with persistent heart pain, interruptions in its functioning, shortness of breath, and pain in the joints. The temperature may rise slightly. As the infectious process progresses, the symptoms become more acute. The heart increases in size, the rhythm of heart contractions is disrupted;
- Idiopathic– has a more severe form, often with a malignant course. Characteristic symptoms: heart enlargement, beating rhythm is greatly disturbed. Complications are possible in the form of blood clots, heart failure, thromboembolism and;
- Allergic– occurs 12 hours to 2 days after the vaccine or drug that provokes an allergy in the patient was administered. In rheumatism and connective tissue pathologies, myocarditis is a symptom of the underlying disease.
There are the following forms of the disease:
- With the flow: acute myocarditis in children, subacute, chronic;
- According to the prevalence of inflammation: isolated and diffuse;
- By severity: degree mild, moderate and severe;
- According to clinical manifestations: erased, typical, asymptomatic forms.
Causes
The reasons for the development of early age myocarditis are varied and are caused by the influence of various factors.
- Infections: bacterial, viral, fungal, spirochetal, rickettsial, caused by protozoa.
- Worm infestations for: trichinosis, cysticercosis, echinococcosis.
- Toxic, chemical factors : wasp bite, snake bite, exposure to mercury, carbon monoxide, arsenic, drug and alcohol use.
- Physical factors: hypothermia, ionizing radiation, overheating.
- Impact medicines : sulfonamide drugs, antibiotics, vaccines, serums, spironolactone.
Myocarditis often develops in children with rheumatism, diphtheria, and scarlet fever. The disease is noted at the moment allergic reactions, when exposed to toxins, congenital. With autoimmune myocarditis, the child’s body produces antibodies to the cells of the heart muscle.
By origin, the disease can be of a rheumatic or non-rheumatic nature.
Rheumatic myocarditis develops as a result. Non-rheumatic myocarditis is caused by inflammatory processes of different nature. The non-rheumatic form often appears after or.
Rheumatic myocarditis has both acute and chronic form. Has symptoms such as general weakness, mood swings. If there are no changes in the heart area, then a lot of time sometimes passes before a disease such as rheumatic myocarditis is identified. It has the first symptoms such as shortness of breath during physical activity, strange sensations in the heart area.
Symptoms
There is no clinical symptom that would allow one hundred percent accuracy to diagnose myocarditis– this disease in children is characterized by severity and a rapid increase in existing symptoms. Symptoms of the clinical manifestation of the disease may vary depending on:
- Immediate cause;
- Depth of damage;
- The extent of inflammation in the heart muscle;
- A certain flow variant.
The prevalence of inflammation has an impact on the clinical manifestations of this disease. At the neonatal stage (4 weeks after the birth of the child), congenital myocarditis is severe and has the following symptoms:
- The skin is pale with a gray tint;
- Weakness;
- Weight gain is very slow.
Symptoms such as palpitations and shortness of breath appear during bathing, feeding, defecation, and changing. Swelling may also occur. The liver and spleen enlarge. There is a reduction in the daily amount of urine.
In infants, the disease usually develops against the background of an ongoing infection or after a week. The temperature rises to 37.5° C, and sometimes higher.

Myocarditis in infants may well begin with shortness of breath. Initial symptoms in children after 2 years of age are severe abdominal pain. The baby's hands and feet become cold. The child is lethargic. There is an enlargement of the heart and liver. The child has a delay in physical development. A dry cough may occur.
In severe cases, symptoms such as fever and swelling in the alveoli of the lungs may appear, which can result in death.
In older age, the disease occurs in acute, subacute, chronic recurrent form, and has a more benign course. After past infection Myocarditis has no symptoms within 2-3 weeks. After which symptoms such as weakness, fatigue, pale skin, and weight loss appear.
The temperature may be normal or slightly increased. Children may be bothered by joints and muscles.
Children of preschool and school age experience heart pain and shortness of breath. Initially, these appear during physical activity, then at rest. The pain in the heart is not pronounced, but it is long-lasting and difficult to relieve with medications. Rapid heartbeat and expansion of the borders of the heart are noted less frequently. But heart rhythm disturbances, swelling in the extremities, and enlarged liver may appear.
Diagnostics
For diagnosis, 24-hour Holter ECG monitoring is used. Echocardiography allows you to determine the size of the heart cavities. Diagnosis of myocarditis has major and minor criteria. It is imperative to identify 1-2 major or 2 minor criteria, as well as anamnesis.
Diagnostics uses antimyosin scintigraphy or gallium techniques, as well as magnetic resonance with gadolinium.
Diagnosis is especially difficult in the absence of clear specific diagnostic criteria.
According to clinical guidelines Treatment of acute myocarditis in children is carried out in a hospital. Characterized by strict bed rest, the duration of which is determined individually. Bed rest is also required in the absence of manifestations of heart failure. Severe cases are characterized by the use of oxygen therapy.

Treatment of myocarditis must be comprehensive. No specific treatment has been developed. The main focus is the treatment of the disease that caused this heart disease.
The main components of complex therapy for the disease are:
- For bacterial infections, antibiotics are used (Doxycycline, Monocycline, Oxacillin, Penicillin);
- For myocarditis caused viral infection, antiviral drugs are used (Interferon, Ribavirin, Immunoglobulins). An immunomodulator is often prescribed without side effects and contraindications.
With intravenous administration of gammaglobulin, the survival rate of children increases and the recovery of myocardial function improves.
Complex treatment includes such anti-inflammatory non-steroidal drugs , such as: salicylates and pyrazolone drugs (Indomethacin, acetylsalicylic acid, Methindol, Butadione, Brufen, Hydroxychloroquine). Such drugs are mandatory in the treatment of a disease with a protracted or recurrent course. Some of these medications relieve heart pain.
For persistent pain, Anaprilin is prescribed minimum dose. Hormonal drugs such as glucocorticoids have a powerful anti-inflammatory and anti-allergic effect. Prednisolone, Dexamethasone, Hydrocortisone, Triamcinolone are used to treat severe forms of the disease. Hormonal therapy is applicable for heart failure, autoimmune myocarditis,. The dosage and duration of use of hormones is determined individually.
During treatment hormonal agents Potassium supplements are prescribed; the following foods are rich in it: dried apricots, raisins, carrots.
In case of heart failure, after stopping inflammation in the myocardium, digitalis preparations are used. In case of severe deficiency, Dopamine and Dobutamine are used. And for edematous syndrome, such drugs as Hypothiazide, Fonurit, Novurit, Lasix, and a fasting diet are applicable. Complex treatment must include vitamin preparations: B vitamins, . For anxiety, headaches, and sleep disturbances, symptomatic treatment is provided.
If the rhythm of cardiac activity is disturbed, antiarrhythmic drugs are selected. For persistent arrhythmias, a surgical treatment method is performed: transvenous cardiac pacing or implantation of a pacemaker. In case of chronic recurrent myocarditis after hospital treatment, regular preventive trips to a specialized sanatorium are recommended.
