Sexual organism of women. Three types of female reproductive organs
In general, we can say: the female genital organs are absolutely individual. Their size, color, location, shapes create unique combinations.
But even here there is a classification.
For example, according to the location of the vulva
- The one closest to the navel is called the "English lady".
- If the vagina is closer to the anus, then this is a "minx".
- And those who have taken a strictly middle position are called "queens".
Many peoples have their own names for different sizes of the vagina.
So, in tantric sexology there are three main types.
- The first is a deer (no deeper than 12.5 centimeters). The female fallow deer has a tender, girlish body, firm breasts and hips, is well built, eats in moderation, and loves to have sex.
- The second is a mare (no deeper than 17.5 centimeters). The female mare has a slender body, lush breasts and hips, and a noticeable belly. This is a very flexible, graceful and loving woman.
- The third type is the elephant (up to 25 centimeters deep). She has large breasts, a broad face, short arms and legs, and a deep, rough voice.
Poetic comparisons of the vulva by the appearance of the labia are known, which can also be considered a kind of classification: rosebud, lily, dahlia, aster and tea rose ...
A peculiar (to put it mildly) “classification” of vaginas is given in the book of the Polish author M. Kinessa (there are still disputes about whether he really existed) “Marriage under a microscope. Physiology of human sexual life»
Here is what he writes, referring to a certain Professor Jacobson
In addition to the topographic position of the slit /queenie (wren), sips, patties/, the genitals of women also differ in the size of the vagina /length, width/, the position of the clitoris, relative to the vagina /high, low/, the size of the clitoris /large, small/, size and the design of the labia, especially the small ones, the degree of moistening of the vagina with juice during sexual arousal /dry and excessively moistened vagina/, as well as the plane in which the genital tube of the woman is compressed.
The classification is as follows:
VIRGIN - untouched by men, the genitals of a girl / in Polish "Pervachka" /.
DICCHKA - a sexual organ with an extensible hymen, which persists until childbirth.
CHILEAN - the genitals of a girl without a hymen. Found in India, Brazil, Chile. This is explained by the fact that mothers in these countries wash little girls so vigorously that the hymen is completely destroyed even in early childhood.
EVE - vulva with a large clitoris /6-8 cm or more/, women with a large clitoris are less intelligent, but more sensitive.
MILKA - a vulva with a clitoris located close to the entrance to the vagina / low / and rubbing during intercourse directly with the penis of a man. Women with Milka are easily satisfied, during sexual intercourse they almost do not require caresses.
PEAHEN - vulva with a high located clitoris. During intercourse, such a vulva is extremely in need of caresses, since her clitoris does not rub directly against the man's penis / but rubs against other parts of the man's body, which greatly reduces feelings /.
ZAMAZULIA - vulva with copious secretion of juice during sexual arousal of a woman. Causes discomfort in a sexual partner and often leads a man to refuse copulation.
KOSTYANKA - an underdeveloped flat external organ of a woman with infantile labia. It occurs, as a rule, in thin women with a narrow pelvis, almost all Kostyanka are Sipovki, that is, they have a low location of the genitals. The drupe is one of the most unattractive genital organs for men.
MONKEY - the sexual organ of a woman with an abnormally long clitoris, more than 3 cm. It is so named because in some monkeys the clitoris reaches a length of 7 cm and is often longer than the penis of a male.
HOTTENDOT APRON - the genital organ of a woman with overdeveloped labia, covering the entrance to the vagina and hanging outside the labia majora. Such an organ pathology can develop as a result of excessive female onanism on the labia.
PRINCESS - the most beautiful female genital organ with a well-developed clitoris, small labia in the form of a pink flower bud above the entrance to the vagina. The princess is the most beloved by men, the most attractive and convenient for intercourse in any position is the sexual organ of a woman. With good hormonal secretion, a woman who has a princess is able to receive and deliver unspeakable pleasure to a man. In addition, the small size of the genital tube, which also attracts men. The princess is found only in short / but medium-sized women inclusive / women with full hips, developed breasts and a wide pelvis.
The semi-princess, semi-drugs, semi-events, etc. organs occupy an intermediate position.
This classification of the appearance of the vulva. Some authors also mention transverse vulvas, "Mongolian type" vulvas. But no less important for the course of sexual intercourse is the size of the genital organs of women.
These dimensions are described by the following classification:
Manilka - vagina up to 7 cm long /attracts men/
Swan - 8–9 cm
Guinea fowl - 10 cm
fool - 11–12 cm
Manda - 13 cm or more.
in width:
Khmelevka - vagina 2.5 cm wide /gives men hops/
Enchantress - 3 cm /charms men/
Slastunya - 3.5 cm / softens during intercourse /
Lyubava - 4 cm
hetaera - - 5 cm and more / so they called prostitutes in ancient times /.
Sexologists use the following terminology:
Bacchante - a female organ with easily excitable erogenous zones, always having a desire for caresses. Such an organ is popularly called a “hot vulva” / in Georgian, tskheli muteli /.
forget-me-not - a female organ that has not given birth.
Bride - a vulva-one-man, that is, a female organ that knew the caress of only one man.
Chamomile - the sexual organ of the girl before the onset of the first menstruation and hair growth.
Madonna - This is the vulva that has experienced sexual intercourse for the first time.
drinker - the sexual organ of a depraved woman.
About the distribution of one or another type of female genital organ

I will make a reservation in advance that the frequency with which this or that type of female vulva occurs is different in different peoples. The names of the vulvae given by me, depending on the length and width of the vagina, are valid for the peoples of Europe, including Greece, France, Spain, Italy, Germany, the Czech Republic, Slovakia, Poland, and Russia.
They are found in Europe with the following probability:
Eva - one in twenty vulvas, Milka - one in thirty vulvas, Pava - very common, Kostyanka - quite common, in Europe, each of the 6 vulvas Kostyanka, and in some peoples more often, Khmelevka - one in 70 vulvas, Manilka - one for 90 vulvas, Swan - one for 12 vulvas, Enchantress - one for 15 vulvas. As for the Princess - the most charming female organ, looking at which even women experience aesthetic pleasure, not to mention men, they meet with a probability of one in 50 vulvas.
Sexologists, however, note that in some nations one or another type of female organ may predominate. So, for example, it is no secret that narrow and short vaginas predominate in Greek, French and Italian women (among them there is a high percentage of Khmelevok, Manilok, Swans, Charodeeks).
Women of African nationalities, as well as black women and mulattos of the American continent, are dominated by long vaginas. Among Georgians, Spanish women and German women, drupes predominate. It can be added that in every nation all the types of genital organs described above are necessarily found.
Modern sexologists say that the vaginotherory described in the above book is a kind of processing of Soviet (to a greater extent) and Polish (to a lesser extent) tales and fabrications about the female genital organ.
But some young men and young men in the post-Soviet space (and one should not think that there are so few of them) are still “afraid” of Kostyanka and the Gottendot apron and secretly dream of finding the Princess with this or that beauty. So do not be surprised if it suddenly turns out that for you the Kinglet is a songbird, and for him - a woman whose vagina is located at the point as far as possible from the anus, almost in the lower abdomen!
The external genitalia include the pubis, labia majora and labia minora, and the clitoris.
Figure: External genitalia.
1 - pubis; 2 - head of the clitoris; 3 - big lips; 4 - external opening of the urethra; 5 - hymen; 6 - navicular fossa; 7 - perineum; 8 - posterior commissure of the lips; 9 - opening of the excretory duct Bartol. glands; 10 - entrance to the vagina; 11 - paraurethral course; 12 - small lip; 13 - frenulum of the clitoris; 14 - the foreskin of the clitoris.
The hymen is the boundary between the external and internal genital organs.
The pubis (mons veneris) is a border area of the abdominal wall, somewhat elevated due to the abundance of subcutaneous fat. The skin of the pubis is covered with hair, the upper border of which ends horizontally (“according to the female type”). In men, the upper border of hairiness is pointed upward along the midline of the abdomen, sometimes reaching the navel. An abundance of hair in women (hirsutism) occurs with infantilism, ovarian tumors, and anomalies in the hormonal function of the adrenal glands. Above the bosom, 1-2 cm above the edge of the hairline, a skin groove curved downwards is determined, convenient for transverse incision.
Large labia (labia majora) - thick skin folds with abundant fatty lining, pigmented, covered with hair and containing sweat and sebaceous glands. Their inner edge is very delicate, hairless and approaches the structure of the mucous membranes. In front, the large lips pass into the skin of the pubis, forming the anterior commissure (commissura ant.) of the lips; posteriorly, they converge into a thin fold - the posterior commissure (commissura poster). Pulling the posterior commissure, you can find the space between it and the hymen - the navicular fossa (fossa navicularis).
In the thickness of the large lips lies a significant layer of fatty tissue, in which venous plexuses, bundles of fibrous tissue and elastic fibers are found. At the base of the large lips lie the Bartholin glands and bulbs of the vestibule (bulbi vestibuli). In front of the lips there are round uterine ligaments emerging through the inguinal canal and crumbling in the thickness of the lips. A volvulus of the peritoneum, which sometimes goes along with the round ligament, the Nucco canal, can sometimes serve as a source of labial hernias, as well as hydrocelefeminina; the latter was observed in 1960 in the clinic of the Crimean Medical Institute.
Small labia (labia minora) - delicate structure of skin folds, similar to the mucous membrane, located medially from the large lips. Posteriorly, the small lips merge with the large ones. Anteriorly bifurcating, they form the foreskin and frenulum of the clitoris. Small lips are covered with stratified squamous epithelium, have sebaceous glands, but do not contain hair, sweat and mucous glands. A rich supply of nerve endings and blood vessels contributes to erectility and great sensitivity of the small lips.
The clitoris (clitoris, cunnus) is formed from two cavernous bodies covered with m. ischiocavernosus. Under the symphysis, the legs of the clitoris, merging into one body, thicken, forming the head of the clitoris (glans clitoridis). From below, under the clitoris, there is a frenulum (frenulum clitoridis), passing into the inner edges of the small lips. The clitoris contains many sebaceous glands that secrete smegma; it is also rich in nerve endings ("Dogel's bodies") and is very sensitive.
Below the clitoris is the external opening of the urethra, surrounded by a small roller, on both sides of which you can find 2-4 openings of the canal passages; in the latter, persistent foci of female gonorrhea are most often observed.
The female urethra is short (3-4 cm), not convoluted, its mucous membrane forms a longitudinal folding. The muscular layer of the urethra consists of external circular fibers and internal - longitudinal. Circular muscles form the internal urethral sphincter near the bladder, the external sphincter is formed by striated fibers of the urogenital diaphragm.
Bartholin's glands, or large vestibular glands (glandulae vestibul. majores), are located in the lower third of the thickness of the large lips between the bulbus vestibuli and m. levat. ani, and their excretory duct opens at the base of the small lips, between them and the hymen, on the border of the middle and lower parts of the genital slit. In contrast to Skene's ducts, Bartholin's glands are true glands with significant pimple-like ramifications and secerating epithelium. The excretory ducts of these glands open on the mucous membrane of the vestibule with two punctate depressions. They are easy to recognize when squeezing out the secret with the index and thumb, the first of which is inserted into the vagina; at the same time, a drop of secret appears from the opening of the excretory duct.
The hymen (hymen) is a connective tissue membrane. The shape of the hymen can be annular, semi-lunar, lobed, trellised. Tears of the hymen - carunculae hymenales - are formed during the first sexual intercourse, but its significant destruction occurs only during childbirth, when papilla-like formations remain from it - carunculae myrtiformes.
If you push the labia apart, then a space is found that is called the vestibule (vestibulum). It is bounded anteriorly by the clitoris, laterally by the small lips, and posteriorly by the navicular fossa. In the center of the vestibule, the entrance to the vagina (introitus vaginae) opens, surrounded by the remains of the hymen or half-closed by it.
Perineum (perineum) - soft tissues of the skin, muscles and fascia, located between the rectum and the vagina and limited laterally by the ischial tubercles. The part of the perineum between the coccyx and the anus is called the posterior perineum.
The vagina (vagina, colpos) is an internal genital organ, an elastically extensible tube connecting the cervix to the genital slit. Its length is about 10 cm.

Figure: A woman's vagina opened lengthwise (E. N. Petrova).
The lumen of the vagina is narrower in the lower section; in the middle part of its wall fall off in the anteroposterior direction. At the top, the vagina expands, forming its arches (anterior, posterior and lateral). Of these, the posterior arch (fornix posterior) is especially pronounced. The vaults surround the vaginal part of the cervix. The vaginal mucosa is covered with stratified squamous epithelium. To the mucosa, devoid of a submucosal layer, the muscular layer is directly adjacent, consisting of an inner layer of circular fibers and an outer layer of longitudinal muscle fibers, rich in elastic elements. The vagina is devoid of glands. Its discharge consists of transudate, desquamated epithelium and gram-positive rods (Dederlein). The reaction of the discharge of the vagina in healthy women is acidic due to the formation of lactic acid from the glycogen of the cells of the vagina; the concentration of lactic acid in the discharge is 0.3%.
The uterus (uterus) is pear-shaped, 8-9 cm long, flattened in the anteroposterior direction. It distinguishes the body, isthmus and neck. 
Figure: Sagittal section of the uterus giving birth.
1 - supravaginal part; 2 - isthmus; 3 - middle part; 4 - vaginal part.
The body of the uterus is divided into the bottom of the uterus and the body itself. In the neck, the supravaginal part, the middle part (between the place of attachment of both arches) and the vaginal part are distinguished. The isthmus is the narrow belt of the uterus between the supravaginal part and its body; during pregnancy and childbirth, it expands into the lower segment. The vaginal part of the cervix (portio vaginalis uteri) is covered with a multi-layered, flat, glycogen-containing epithelium, the same type as the epithelium of the vagina. The stroma of the mucous membrane of the vaginal part of the cervix consists of loose connective tissue with many round cells, rich in blood vessels. The arteries of the neck go in the radial direction, passing under the mucosal layer into the capillary network; veins and lymphatic vessels are also located there. The boundary between the stratified squamous epithelium of the vaginal part of the cervix and the columnar epithelium of the cervical canal is very variable.
The cervical canal has a fusiform shape, and the middle of the canal is wider than its internal or external os. The inner surface of the canal is covered with significantly pronounced oblique mucosal folds, the thickness of which reaches 2 mm. In an oblique direction, a large number of glands with a tubular structure pass through the thickness of the cervical mucosa. These glands are able to grow into the muscles of the neck. The mucous secretion of the cervical glands has an alkaline reaction. The epithelium of the cervical canal consists of high cylindrical cells that do not contain glycogen; their nuclei are located basally and are well outlined. At the peripheral end, epithelial cells (but not all) are provided with cilia. The epithelium of the glands also consists of cylindrical cells, partially provided with cilia. The overall picture of the glands (at low magnification) represents individual fluctuations. The glands can be distributed evenly throughout the cervical canal or grouped in separate parts of it.
At the lower end of the vaginal part of the cervix there is an external opening, or external pharynx (orificium externum), which opens into the vagina.
In nulliparous, the external pharynx has a rounded shape, in those who have given birth, it has the shape of a transverse slit; it divides the neck into two lips: anterior and posterior. 
Figure: a - the pharynx of a nulliparous woman; b - pharynx of a woman giving birth.
The uterine cavity is a triangular slit, the upper corners of which correspond to the mouths of the tubes, and the lower corner corresponds to the internal opening of the cervix (orificium internum). 
Figure: The uterine cavity of a nulliparous woman. 
Figure: The uterine cavity of a woman giving birth.
The wall of the uterus consists of three layers: perimetrium, myometrium and endometrium. The endometrium has a smooth surface and becomes thinner towards the internal os. The mucous membrane of the inner wall of the uterus is covered with a cylindrical epithelium, partly with ciliated hairs, and is replete with glands. These glands, unlike the cervical ones, have a different shape depending on the stage of the menstrual cycle: in the proliferation phase they are tubular, in the secretory they become convoluted, corkscrew. They have almost no external secretion. The mucosa of the body of the uterus consists of two layers: the superficial - functional, changing in different phases of the menstrual cycle, and the deep - basal layer, which has not undergone significant changes and is tightly adjacent to the surface of the myometrium. The basal layer consists of a dense connective tissue stroma rich in spindle cells; functional has a looser structure with large star-shaped cells. The location of the glands of the functional layer is correct: from above and outside from top to bottom and inside; in the basal layer, the glands are located incorrectly. The epithelial cells in the glands are low with a large dark nucleus, the remains of the secret are found in the lumen of the glands. The glands of the uterus in some places penetrate the muscle layer.
The architectonics of the uterine myometrium (pregnant and non-pregnant) is complex and was not clear until attempts to explain the structure of the myometrium from a genetic point of view began. There are subserous, supravascular, vascular and submucosal layers of the myometrium. Due to the interweaving of the fibers, the muscle layers are difficult to separate from each other. The vascular layer is the most developed.
By genesis, the direction of the muscle fibers of the human uterus, formed from the fusion of the Mullerian passages, which occurs in the third month of fetal development, is associated with the muscle layers of the fallopian tubes. The outer, longitudinal layer of the tube diverges along the surface of the uterus under its serous cover, and the inner, circular layer provides the basis for the middle muscular layer of the uterus. 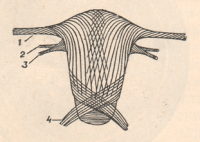
Figure: The outer layer of the muscle fibers of the uterus (scheme).

Figure: The inner layer of the muscle fibers of the uterus (scheme).
1 - pipe; 2 - round ligament; 3 - ovarian ligament; 4 - sacro-uterine ligament.
A lot of smooth muscle fibers from the ligamentous apparatus of the uterus are also woven here in the form of sheaves - the round ligament, the own ligament of the ovary, and especially the sacro-uterine ligaments. The uterus of a woman with malformations can repeat ontogenetically primary or intermediate types of development. So, in the bicornuate uterus of a woman, one can clearly distinguish the outer longitudinal and inner circular layers.
The wall of the body of the uterus consists of well contracting smooth muscle fibers, the neck - of connective tissue with an admixture of a small number of muscle fibers capable of contracting.
According to N. 3. Ivanov, the muscles of the uterus are distributed as follows. 
Figure: The structure of the fibers of the uterine muscle according to N. Z. Ivanov
From the inguinal canals there are bundles of smooth muscles, folded at their beginning into a tourniquet, which is why they are called round ligaments. At the anterior surface of the uterus, the bundles spread into the outer layer of its musculature, 7 mm thick. From the back surface of the layer depart: 1) muscle bundles to the vascular branches a. spermaticae, forming the middle layer of muscles and 2) muscle bundles encircling the uterus and going to its back surface; they are especially pronounced in the thickness of the uterus above the cervix and at the internal pharynx. Many bundles also extend from the anterior surface of the layer into the middle (vascular) layer of the myometrium. These bundles near the midline turn downward, forming a large median bundle in the form of a roller, especially noticeable in the pregnant and postpartum uterus. On the back surface of the uterus, a median bundle (roller) is also formed, but less noticeable. The musculature of the body of the uterus, according to N. 3. Ivanov, is in close connection with the bulk of the muscle fibers of the neck; the latter are a continuation of the outer and vascular layers, and do not begin in the neck itself. 
Figure: The structure of the fibers of the uterine muscle according to N. Z. Ivanov. Sagittal section.
In addition to the main two bundles of muscles coming from the round ligaments, there is a third bundle that goes to the uterus from fascia pelvis and penetrates into the back of the cervix and body of the uterus in the form of a layer, 3-5 mm thick (m. retrouterinus fasciae pelvis). While the first two bundles exhibit many folds and can be traced all the way from the cervix through the body of the uterus to the ligaments, the third bundle represents a separate muscular system, without anastomoses and folds, with a characteristic direction of its fibers from the bottom up. This system was first described by N. 3. Ivanov. Some of its fibers form the sacro-uterine ligaments.
The body of the uterus is covered with peritoneum (perimetrium), which extends to neighboring organs as follows: the peritoneum from the anterior abdominal wall passes to the bottom of the bladder and its posterior wall; then it passes to the anterior wall of the uterus, forming a depression between the bladder and the uterus - excavatiovesicouterina. Then the peritoneum passes to the bottom and back surface of the uterus, and from here to the anterior wall of the rectum. Between the uterus and the rectum, the peritoneum forms a second recess, a deeper one - excavatio rectouterina, or Douglas space. On the side of the uterus, the peritoneum forms a duplication - wide ligaments of the uterus, extending from its ribs to the side walls of the pelvis (lig. lata uteri).
Part of the fiber of the pelvis, located under the broad ligament and, therefore, also extending from the sides of the uterus to the walls of the pelvis, is called periuterine fiber (parametrium). Periuterine tissue - loose connective tissue in which arteries, veins, lymphatic vessels and nerves pass - is part of the entire pelvic tissue.
The fiber of the pelvis, lying between the leaves of the broad ligaments at their base, is dense; these are the main ligaments (lig. cardinalia). From the body of the uterus, slightly below the place of discharge of the tubes, in the folds of the broad ligament, connective tissue strands pass on both sides - round ligaments of the uterus (lig. teres s. rotunda); they pass through the inguinal canal and attach to the pubic bone. The last pair of uterine ligaments are sacro-uterine ligaments (lig. sacrouterina), extending from the posterior wall of the uterus at the level of the internal os. These ligaments, covering the rectum, are attached to the pelvic surface of the sacrum.
The uterine appendages include the uterine or fallopian tube (tuba uterina s. Fallopii), or the oviduct, and the ovary.
The fallopian tube runs from the upper lateral edge of the uterus in the direction of the side wall of the pelvis, and its main bend, crossing the ovary, is turned backwards. 
Figure: Uterus and appendages.
1 - uterus; 2 - pipe; 3 - steamer; 4 - ovary; 5 - the actual ovarian ligament.
There are three main sections of the tube: the interstitial part is the shortest, passing through the thickness of the uterine wall and having the narrowest lumen (less than 1 mm), the isthmus part and the ampullar part. The ampullar part expands into a funnel of the pipe, which splits into fimbriae, or fimbriae; the largest of them is called fimbria ovarica.
The tube is covered with a peritoneum that descends along its sides and forms a duplication below the tube - the mesentery of the tubes (mesosalpinx). The epithelium of the mucous tube is cylindrical ciliated. The tube is capable of peristaltic and anti-peristaltic movements.
The ovary is adjacent to the posterior surface of the broad ligament, attaching to it through a small mesentery (mesovarium); throughout the rest of the length, the ovary is not covered by the peritoneum. The ovary is attached to the pelvic wall by means of a ligament - lig.infundibulopelvicum or lig. suspensorium ovarii; it is connected with the uterus by means of lig. ovarii proprium.
The ovary is covered with germinal epithelium. It distinguishes between the cortical layer containing the follicles and the medulla.
The ovaries are highly mobile and follow the changing position of the uterus. The size of the ovary, which is normally equal to the size of a small plum, can vary in the same woman, increasing during menstruation and by the time the follicle matures.
The arteries that feed the external and internal female genital organs are as follows. 
Figure: Vessels of the female genitalia.
1 - common iliac arteries and vein; 2 - ureter; 3 - hypogastric (internal iliac) artery; 4 - external iliac artery; 5 - uterine artery; 6 - prevesical tissue; 7 - uterus; 8 - round ligament; 9 - ovary; 10 - pipe. 
Figure: Vessels and nerves of the pelvic floor.
1-a. clitoridis; 2-a. bulbi vestibule; 3-a. pudenda int.; 4 - a. haemorrhoid. inf.; 5 - nn. labiales post.; 6 - n. dorsalis clitoridis; 7 - m. levator ani; 8-lig. Sacrotuber; 9-nn. haemorrh. inf.; 10-n. cutan. femor. post.; 11-n. pudendus.
The external genitalia receive blood through the internal and external pudendal arteries and the external spermatic artery.
Artery of the uterus - a. uterina - departs from the hypogastric artery - a. hypogastrica - in the depths of the parauterine tissue. Having reached the rib of the uterus, the artery of the uterus at the level of the internal pharynx gives down the cervical-vaginal branch; its main trunk goes up, reaches the pipe, where it is divided into two branches. One of these branches goes to the bottom of the uterus and anastomoses with the arterial branch of the ovary - a. ovaricae; and the other - to the pipe; the latter anastomoses with a branch of the ovarian artery.
It must be remembered that the artery of the uterus, not reaching 1.5-2 cm to the rib of the latter, crosses with the ureter, located anterior to it.
The internal seminal artery, or ovarian (a. spermatica int. s. ovarica), departs from the aorta. From the ovarian artery depart tubal and ovarian branches that feed the corresponding organs.
In addition to these two artery systems, the internal genital organs of a woman receive nutrition from the external seminal artery or the artery of the round ligament (a. spermatica ext., s. a. lig. rotundi) - branches of the inferior epigastric artery).
The vagina is nourished by: the lower cystic artery (a. vesicalisinf.) and the middle rectal - a. haemorrhoidalis media (branches of the hypogastric artery), as well as the internal pudendal artery (a. pudenda int.). Arteries are accompanied by veins of the same name, which form powerful plexuses in the parametrium (cystic, utero-ovarian, and others).
FEMALE GENITAL ORGANS.
1. Internal female genital organs.
2. External female genital organs.
3. The structure of the sexual cycle of a woman.
PURPOSE: To know the topography, structure and functions of the internal female genital organs: ovary, uterus, fallopian tube, vagina and external genitalia: female genital area and clitoris.
Be able to show on posters and tablets the internal and external female genital organs and their individual parts.
Represent the physiological mechanisms of the processes of ovulation, menstruation, the structure of the female sexual cycle.
1. Female reproductive organs are used for the growth and maturation of female germ cells (eggs), gestation and the formation of female sex hormones. According to their position, the female genital organs are divided into internal (ovaries, uterus, fallopian tubes, vagina) and external (female genital area and clitoris). The branch of medicine that studies the characteristics of the female body and diseases associated with a violation of the activity of the genital organs is called gynecology (Greek qyne, qynaikos - woman).
Ovary (ovarium; Greek oophoron) is a paired gonad that produces female sex cells and hormones. It has the shape of a flattened oval body 2.5-5.5 cm long, 1.5-3 cm wide, up to 2 cm thick. pelvis, and lateral, adjacent to the wall of the small pelvis, as well as the upper tubal and lower uterine ends, the free (posterior) and mesenteric (anterior) edges.
The ovary is located vertically in the pelvic cavity on both sides of the uterus and is attached to the posterior leaf of the broad ligament of the uterus through a small fold of the peritoneum - the mesentery. In the region of this region, vessels and nerves enter the ovary, therefore it is called the gate of the ovary. One of the fimbriae of the fallopian tube is attached to the tubal end of the ovary. From the uterine end of the ovary to the uterus goes its own ligament of the ovary.
The ovary is not covered by the peritoneum; on the outside there is a single-layer cubic epithelium, under which lies a dense connective tissue albuginea. This ovarian tissue forms its stroma. The substance of the ovary, its parenchyma, is divided into two layers: the outer, more dense, - the cortical substance and the inner - the medulla. In the medulla, which lies in the center of the ovary, closer to its gates, numerous vessels and nerves are located in the loose connective tissue. In addition to the connective tissue, the cortical substance located outside contains a large number of primary (primordial) ovarian follicles, in which germinal eggs are located. In a newborn, the cortex contains up to 800,000 primary ovarian follicles (in both ovaries). After birth, these follicles reverse development and resorption, and by the onset of puberty (13-14 years), 10,000 of them remain in each ovary. During this period, egg maturation begins in turn. Primary follicles turn into mature follicles - Graafian vesicles. The cells of the walls of a maturing follicle perform an endocrine function: they produce and secrete into the blood the female sex hormone - estrogen (estradiol), which promotes the maturation of follicles and the development of the menstrual cycle.
The cavity of a mature follicle is filled with fluid, inside which an ovum is located on the oviduct. Regularly after 28 days, another mature follicle ruptures, and with the flow of fluid, the egg enters the peritoneal cavity, then into the fallopian tube, where it matures. The rupture of the mature follicle and the release of the egg from the ovary is called ovulation. A corpus luteum forms at the site of the ruptured follicle. It plays the role of an endocrine gland: it produces the hormone progesterone, which ensures the development of the embryo. There are menstrual (cyclic) corpus luteum and corpus luteum of pregnancy. The first is formed if the fertilization of the egg does not occur, it functions for about two weeks. The second is formed at the onset of fertilization and functions for a long time (throughout the entire pregnancy). After atrophy of the corpus luteum, a connective tissue scar remains in its place - a whitish body.
Another process in a woman's body is associated with ovulation - menstruation: periodic discharge from the uterus of blood, mucus and cellular detritus (decay products of dead tissues), which are observed in a sexually mature non-pregnant woman after about 4 weeks. Menstruation begins at the age of 13-14 and lasts 3-5 days. Ovulation precedes menstruation by 14 days, i.e. it occurs in the middle between two periods. By the age of 45-50, a woman has a menopause (menopause), during which the processes of ovulation and menstruation stop and menopause occurs. Before the onset of menopause, women have time to mature from 400 to 500 eggs, the rest die, and their follicles undergo reverse development.
The uterus (uterus; Greek metra) is an unpaired hollow muscular organ designed for the development and bearing of the fetus during pregnancy and its excretion during childbirth. It is located in the cavity of the small pelvis between the bladder in front and the rectum in the back, has a pear-shaped shape. It distinguishes: the bottom, facing up and anteriorly, the body - the middle part and the neck facing down. The place of transition of the body of the uterus into the cervix is narrowed (isthmus of the uterus). In the body of the uterus there is a cavity, which communicates with the fallopian tubes from the bottom side, and in the cervical region passes into the cervical canal. The cervical canal opens with a hole in the vagina. The length of the uterus in an adult woman is 7-8 cm, the width is 4 cm, the thickness is 2-3 cm, the weight in nulliparous women is 40-50 g, in those who have given birth up to 80-90 g, the volume of the cavity is 4- 6 cm3.
The wall of the uterus is very thick and consists of three membranes (layers):
1) internal - mucous, or endometrium; 2) middle - smooth muscle, or myometrium;
3) external - serous, or perimetry. Around the cervix, under the peritoneum, there is periuterine fiber - parametrium.
The mucous membrane (endometrium) forms the inner layer of the uterine wall, its thickness is up to 3 mm. It is covered with a single layer of cylindrical epithelium and contains the uterine glands. The muscular membrane (myometrium) is the most powerful, built from smooth muscle tissue, consists of inner and outer oblique and middle circular (circular) layers, which are intertwined with each other. Contains a large number of blood vessels. Serous membrane (perimetry) - the peritoneum covers the entire uterus, with the exception of part of the cervix. The uterus has a ligamentous apparatus, with the help of which it is suspended and fixed in a curved position, as a result of which its body is tilted above the anterior surface of the bladder. The composition of the ligamentous apparatus includes the following paired ligaments: wide, round ligaments of the uterus, recto-uterine and sacro-uterine.
The uterine (fallopian) tube, or oviduct (tuba uterina; Greek salpinx), is a paired tubular formation 10-12 cm long, through which the egg is released into the uterus. In the fallopian tube, the fertilization of the egg and the initial stages of embryo development take place. Pipe clearance 2 - 4 mm. It is located in the pelvic cavity on the side of the uterus in the upper part of the broad ligament. One end of the fallopian tube is connected to the uterus, the other is expanded into a funnel and faces the ovary. In the fallopian tube, 4 parts are distinguished: 1) the uterine, which is enclosed in the thickness of the uterine wall; 2) the isthmus is the narrowest and thickest part of the tube, which is located between the sheets of the broad ligament of the uterus; 3) the ampulla, which accounts for half the length of the entire uterine pipes; 4) a funnel that ends with long and narrow fringes of the pipe.
Through the openings of the fallopian tubes, uterus and vagina, the peritoneal cavity in women communicates with the external environment, therefore, if hygiene conditions are not observed, infection may enter the internal genital organs and the peritoneal cavity.
The wall of the fallopian tube is formed by: 1) a mucous membrane covered with a single-layer cylindrical ciliated epithelium; 2) a smooth muscle membrane, represented by the outer longitudinal and inner circular (circular) layers; 3) a serous membrane - a part of the peritoneum that forms the broad ligament of the uterus.
The vagina (vagina; Greek colpos) is the organ of copulation. It is an extensible muscular-fibrous tube 8-10 cm long, with a wall thickness of 3 mm. The upper end of the vagina starts from the cervix, goes down, penetrates the urogenital diaphragm and the lower end opens into the vestibule with a vaginal opening. In girls, the opening of the vagina is closed by the hymen (gymen), the place of attachment of which delimits the vestibule from the vagina. The hymen attaches a semilunar or perforated plate of the mucous membrane. During the first intercourse, the hymen ruptures and its remnants form hymen flaps. Rupture (defloration) is accompanied by slight bleeding.
In front of the vagina are the bladder and urethra, and behind the rectum. The vaginal wall consists of three membranes: 1) outer - adventitious, from loose connective tissue containing a large number of elastic fibers; 2) middle - smooth muscle, from longitudinally oriented bundles of muscle cells, as well as bundles having a circular direction; 3) internal - mucous covered with non-keratinized stratified squamous epithelium and devoid of glands. The cells of the surface layer of the epithelium of the mucous membrane are rich in glycogen, which, under the influence of microbes living in the vagina, breaks down to form lactic acid. This gives the vaginal mucus an acidic reaction and determines its bactericidal activity against pathogenic microbes.
Inflammation of the ovary - oophoritis, uterine mucosa - endometritis, fallopian tube - salpingitis, vagina - vaginitis (colpitis).
2. The external female genital organs are located in the anterior perineum in the area of the genitourinary triangle and include the female genital area and the clitoris.
The female genital area includes the pubis, large and small labia, the vestibule of the vagina, the large, small glands of the vestibule and the bulb of the vestibule.
1) The pubis (mons pubis) at the top is separated from the abdomen by the pubic groove, and from the hips by the hip grooves. The pubis (pubic eminence) is covered with hair that continues onto the labia majora. The subcutaneous fat layer is well developed in the pubic area. 2) The labia majora (labia majora pudendi) is a rounded paired skin fold 7-8 cm long, 2-3 cm wide, containing a large amount of adipose tissue. The labia majora limit the genital slit from the sides and are connected to each other by the anterior (in the pubic area) and the posterior (in front of the anus) adhesions. 3) Labia minora (labia minora pudendi) - paired longitudinal skin folds. They are located medially and are hidden in the genital gap between the labia majora, limiting the vestibule of the vagina. The labia minora is built from connective tissue without adipose tissue, contains a large number of elastic fibers, muscle cells and venous plexuses. The posterior ends of the labia minora are connected to each other by a transverse fold - the frenulum of the labia, and the upper ends form the frenulum and the foreskin of the clitoris. 4) The vestibule of the vagina (vestibulum vaginae) is the space between the labia minora. The external opening of the urethra, the opening of the vagina and the openings of the ducts of large and small vestibular glands open into it. Located on each side at the base of the labia minora, the ducts of both glands open here. A mucus-like liquid is secreted that moistens the wall of the entrance to the vagina. 6) Small vestibular glands (glandulae vestibularis minores) are located in the thickness of the walls of the vestibule of the vagina, where their ducts open. 7) The bulb of the vestibule (bulbus vestibuli) is identical in development and structure to the unpaired spongy body male penis. This is an unpaired formation, consisting of two - right and left parts, which are connected by a small intermediate part of the bulb, located between the clitoris and the external opening of the urethra.
Clitoris (clitoris) - a small finger-shaped elevation 2-4 cm long in front of the labia minora. It distinguishes the head, body and legs, attached to the lower branches of the pubic bones. The clitoris consists of two cavernous bodies, corresponding to the cavernous bodies of the male penis, and contains a large number of receptors. The body of the clitoris is covered on the outside with a dense protein membrane. Irritation of the clitoris causes a feeling of sexual arousal.
3. The sexual cycle of a woman, despite the similarity in the course of the main stages (phases) with the sexual cycle of a man, has specific features. In women, both the duration and intensity of the sexual cycle are much more diverse than in men. This is due to differences in the structure of sexual (sexual - lat. secsus - gender) feelings of men and women. Sexual feeling is the sum of two components (components): the spiritual baggage (wealth) of the individual - the ability to compassion, pity, love, friendship, (the spiritual psychological component of sexual feeling) and sensual erotic (Greek erotikos - love) satisfaction (sensual erotic component ). In the structure of the sexual feelings of men and women, these components are ambiguous. If for men in the structure of sexual feeling the sensual erotic component is in the first place and only the spiritual component is in the second place, then for women, on the contrary, the spiritual component is in the first place and the sensual erotic component is in the second place (a man falls in love with his eyes, and a woman falls in love with her ears). .A man needs a woman's body, and a woman needs a man's soul).
Sexologists conventionally divide women according to sexual feelings into 4 groups:
1) the zero group - constitutionally frigid, who lack a sensual erotic component of sexual feeling; 2) the first group - with a sensual erotic component, but it emerges very rarely among them; this group needs spiritual attunement; 3) the second group - erotically tuned: they also need spiritual attunement, and they experience joy even without orgasm, i.e. without sensual satisfaction; 4) the third group - women who necessarily achieve sensual satisfaction, t .e. orgasm. This group should not include women with a painful increase in sexual desire due to endocrine, nervous or mental disorders.
The first three groups of women can only be content with the spiritual component without orgasmic sensations. The fourth group achieves necessarily orgastic sensations, not content with the spiritual component.
Phase I of the sexual cycle - sexual arousal leads to changes in the external and internal genital organs of a woman in a reflex and psychogenic way. Large and small labia, the clitoris and its head overflow with blood and increase. 10-30 s after sensory or psychogenic arousal, extravasation of the mucous fluid begins through the squamous epithelium of the vagina. The vagina is moistened, which contributes to adequate excitation of the receptors of the penis during coitus. Transudation is accompanied by expansion and lengthening of the vagina. As excitation increases in the lower third of the vagina, as a result of local stagnation of blood, a narrowing (orgasmic cuff) occurs, due to this, as well as swelling of the labia minora, a long canal is formed in the vagina, the anatomical structure of which creates optimal conditions for the occurrence of orgasm in both partners. During orgasm, depending on its intensity, 3-15 contractions of the orgasmic cuff are observed (analogous to emission and ejaculation in men). During orgasm, regular contractions of the uterus are observed, which start from its bottom and cover its entire body, down to the lower sections.
LECTURE №44.
FUNCTIONAL ANATOMY OF THE IMMUNE SYSTEM ORGANS.
1. General characteristics of the organs of the immune system.
2. Central and peripheral organs of the immune system and their functions.
3. The main regularities of the structure and development of the organs of the immune system.
PURPOSE: To know the general characteristics of the immune system, the topography of the organs of the immune system in the human body, the functions of the central and peripheral organs of the immune system.
Represent the main patterns of the structure and development of the organs of the immune system.
1. Immune system - a set of lymphoid tissues and organs of the body that provides protection for the body from genetically alien cells or substances coming from outside or formed in the body. The organs of the immune system, containing lymphoid tissue, perform the function of protecting the constancy of the internal environment (homeostasis) throughout life. They produce immunocompetent cells, primarily lymphocytes, as well as plasma cells, include them in the immune process, ensure the recognition and destruction of cells that have entered the body or formed in it and other foreign substances that carry signs of genetically alien information. Genetic control is carried out by populations of T- and B-lymphocytes that function together, which, with the participation of macrophages, provide an immune response in the body.
The immune system has 3 morphofunctional features: 1) generalized throughout the body; 2) cells constantly circulate through the bloodstream; 3) able to produce specific antibodies against each antigen.
The immune system includes organs that have lymphoid tissue. In the lymphoid tissue, 2 components are distinguished: 1) stroma - a reticular supporting connective tissue consisting of cells and fibers; 2) cells of the lymphoid series: lymphocytes of varying degrees of maturity, plasma cells, macrophages. The organs of the immune system include: bone marrow, in which lymphoid tissue is closely associated with hematopoietic tissue, thymus (thymus gland), lymph nodes, spleen, accumulations of lymphoid tissue in the walls of the hollow organs of the digestive, respiratory systems and urinary tract (tonsils, group lymphoid plaques, solitary lymphoid nodules). These are the lymphoid organs of immunogenesis.
Sexual intercourse is a mechanism of complex interaction between male and female genital organs. The anatomy of intimacy provides the connection between the egg and sperm, resulting in conception. For a better understanding, let's analyze what happens during sex.
Anatomical features of organs
Before proceeding to consider the anatomy of sexual intercourse, it is necessary to remember how the male and female reproductive systems are arranged. It is also necessary to understand the function of each component of the reproductive system. First, let's look at the genitals of women.
- Ovaries.
These are paired glands located in the pelvic cavity. Their function is to secrete female sex hormones. They also produce the maturation of the egg.
- Fallopian, or uterine, tubes.
The fallopian tubes are a paired tubular structure. With their help, the uterine cavity is connected to the abdominal cavity.
- Uterus.
The hollow organ is a reservoir for carrying the fetus. In the structure of the body, the neck, isthmus and body are distinguished.
Female reproductive system.
- Vagina.
This is a muscular organ, which is a tube that connects to the uterus. When excited, the walls are abundantly lubricated with the secretion of the vaginal and Bartholin glands, as well as with plasma penetrating from the blood vessels. The muscular layer of the organ allows the vagina to stretch to the desired size. This fact of anatomy is important during intercourse and during childbirth.
- Large and small labia.
They are located along the edges of the genital slit, so they cover and protect the vagina. These structures are rich in sensitive nerve endings. The labia minora is well supplied with blood, and during sexual arousal they are filled with blood and slightly increase in size.
- Bartholin glands.
These are the glands of external secretion, which are located in the thickness of the labia majora. Their excretory ducts are located at the junction of the small and large labia, and the secret is necessary to moisten the vestibule of the vagina.
- Clitoris.
This is a small tubercle located in the region of the anterior commissure of the labia minora, its main function is to provide orgasm. During arousal, there is an increase in the clitoris in size and swelling.
The organs of the reproductive system in men are also divided into external and internal. Consider the structure of the male genital organs. Their anatomy is shown below:
- Testicles.
These are paired glands that are located in the scrotum. The function is to produce testosterone and sperm.
- seminal vesicles.
Tubular formations with many hollow chambers. They contain nutrients for spermatozoa to ensure their functioning.
- seminiferous tubules.
Designed for blood supply to the testicles and the withdrawal of the seed from them. Here, spermatozoa are formed from the primary germ cells.
Male reproductive system.- The vas deferens are structures designed to eject sperm.
- Penis.
This is the main organ during sexual intercourse. It consists of two cavernous bodies and one spongy. Anatomically allocate the head and body of the penis. It is important to note that the entire surface of the penis is saturated with sensitive receptors. Therefore, this is the main erogenous zone of men.
- Prostate.
It is one of the main glands of the male body. The prostate is involved in the regulation of sexual performance, is responsible for the quality of sperm.
What Happens During Coitus
For sexual intercourse, both the man and the woman must be in a state of excitement. In a man, this is manifested by the presence of an erect penis, and in a woman, by an increase in vaginal secretion. The development of arousal is promoted not only by physical factors, such as stimulation of erogenous zones. Psychological and sensory factors take part in the formation of preparation for sexual intercourse.
In response to stimulation of certain areas of the brain and spinal cord, men experience an expansion of the blood vessels of the penis. As a result, blood flow increases, filling of the cavernous bodies, and the genital organ increases in size and hardens. It is this mechanism that causes the formation of an erection, which makes it possible for the penis to penetrate the vagina.
In women, during arousal, blood flow to the genitals increases, and the secretion of the glands increases. Through the walls of numerous blood vessels that braid the vagina, the liquid part of the blood plasma seeps into its lumen. This anatomy provides moisture to the vaginal mucosa, which facilitates sexual intercourse. It is worth noting that the normal size of the vagina is about 8 cm, but due to the elasticity at the time of intercourse, the organ can expand, change shape, adjusting to the size of the penis.
For sexual intercourse, both the man and the woman must be in a state of excitement.The very process of inserting the penis into the vagina is an even greater stimulant of sexual activity. Then the man begins to commit frictions. These are reciprocating movements made by the pelvis, as a result of which mutual sexual stimulation occurs. The anatomy of women is arranged in such a way that stimulation of the cervix, vagina and clitoris brings maximum satisfaction. In men, the peak of sexual pleasure is observed with direct irritation of the glans penis.
Sexual intercourse ends with the achievement of orgasm. At the same time, in men, contractions of intimate muscles lead to the release of sperm. Seminal fluid is secreted in several portions. The female reproductive system is such that at the time of orgasm, muscle contractions prevent the outflow of seminal fluid and help move it to the cervix. In the future, the sperm enters the uterine cavity, then from the area of \u200b\u200bits bottom penetrates into the fallopian tubes.
If sexual intercourse occurs during the period of ovulation, then the probability of fertilization of the egg is high. Normally, conception occurs in the fallopian tube, and only then the fertilized egg descends into the uterus, where it attaches.
The physiology of sexual intercourse is a complex process of interaction of all organs of the reproductive system, as well as a cascade of biochemical processes. To understand the mechanism of sexual intercourse, it is necessary to clearly understand how the reproductive system works in men and women. This will help you better understand your feelings and find the key to achieving maximum pleasure for your partner.

Although the male and female genital organs (organa genitalia) perform an identical function and have a common embryonic rudiment, they differ significantly in their structure. Gender is determined by the internal genital organs.
Male reproductive organs
Male genital organs are divided into two groups: 1) internal - testicles with appendages, vas deferens and ejaculatory ducts, seminal vesicles, prostate gland; 2) external - penis and scrotum.
Testicle
The testicle (testis) is a paired organ (Fig. 324) of an oval shape, located in the scrotum. The mass of the testicle is from 15 to 30 g. The left testicle is slightly larger than the right one and lowered below. The testicle is covered with a protein membrane (tunica albuginea) and a visceral sheet of the serous membrane (tunica serosa). The latter is involved in the formation of the serous cavity, which is part of the peritoneal cavity. In the testicle, the upper and lower ends (extremitates superior et inferior), lateral and medial surfaces (facies lateralis et medialis), posterior and anterior edges (margines posterior et inferior) are distinguished. The testicle with its upper end is turned upward and laterally. On the posterior margin are the epididymis (epididymis) and the spermatic cord (funiculus spermaticus). There are also gates through which blood and lymphatic vessels, nerves and seminiferous tubules pass. Connective tissue septa diverge from the perforated and somewhat thickened albuginea of the hilum of the testicle towards the anterior edge, lateral and medial surfaces, dividing the testicular parenchyma into 200-220 lobules (lobuli testis). In the lobule lie 3-4 blindly beginning convoluted seminiferous tubules (tubuli seminiferi contort!); each has a length of 60-90 cm. The seminiferous tubule is a tube, the walls of which contain spermatogenic epithelium, where the formation of male germ cells - spermatozoa (see Initial stages of embryogenesis). The convoluted tubules are oriented in the direction of the gate of the testis and pass into the direct seminiferous tubules (tubuli seminiferi recti), which form a dense network (rete testis). The network of tubules merges into 10-12 efferent tubules (ductuli efferentes testis). The efferent tubules on the posterior edge leave the testicle and participate in the formation of the epididymal head (Fig. 325). Above it, on the testicle, there is its appendage (appendix testis), which represents the remainder of the reduced urinary duct.

epididymis
The epididymis (epididymis) is located on the posterior edge of the testis in the form of a club-shaped body. In it, without clear boundaries, the head, body and tail are distinguished. The tail passes into the vas deferens. Like the testicle, the epididymis is covered with a serous membrane that penetrates between the testicle, head and body of the epididymis, lining a small sinus. The efferent tubules in the epididymis are twisted and collected into separate lobules. On the back surface, starting on the head of the appendage, passes the ductulus epididymidis, into which all the tubules of the lobules of the appendage flow.
On the head of the appendage there is a pendant (appendix epididymidis), which is part of the reduced genital duct.
Age features. The mass of the testicle with the appendage in a newborn is 0.3 g. The testicle grows very slowly until puberty, then it develops rapidly and by the age of 20 its mass reaches 20 g. The lumens of the seminiferous tubules appear by the age of 15-16.
vas deferens
The vas deferens (ductus deferens) is 45-50 cm long and 3 mm in diameter. Consists of mucous, muscular and connective tissue membranes. The vas deferens starts from the tail of the epididymis and ends with the vas deferens in the prostatic urethra. Based on the topographic features, the testicular part (pars testiculars) is distinguished in it, corresponding to the length of the testicle. This part is convoluted and adjacent to the posterior edge of the testis. The cord part (pars funicularis) is enclosed in the spermatic cord, which runs from the upper pole of the testicle to the external opening of the inguinal canal. The inguinal part (pars inguinalis) corresponds to the inguinal canal. The pelvic part (pars pelvina) starts from the internal opening of the inguinal canal and ends at the prostate gland. The pelvic part of the duct is devoid of the choroid plexus and passes under the parietal sheet of the peritoneum of the small pelvis. The end part of the vas deferens near the bottom of the bladder is expanded in the form of an ampulla.
Function. Ripe, but immobile spermatozoa, together with an acidic fluid, are removed from the epididymis through the vas deferens as a result of peristalsis of the duct wall and accumulate in the ampulla of the vas deferens. Here, the liquid in it is partially resorbed.
spermatic cord
The spermatic cord (funiculus spermaticus) is a formation consisting of the vas deferens, testicular arteries, plexus of veins, lymphatic vessels and nerves. The spermatic cord is covered with membranes and has the form of a cord located between the testicle and the internal opening of the inguinal canal. Vessels and nerves in the pelvic cavity leave the spermatic cord and go to the lumbar region, and the remaining vas deferens deviates to the middle and down, descending into the small pelvis. The membranes are most complex in the spermatic cord. This is due to the fact that the testicle, leaving the peritoneal cavity, is immersed in a sac, representing the development of the transformed skin, fascia and muscles of the anterior abdominal wall.
Layers of the anterior abdominal wall, membranes of the spermatic cord and scrotum (Fig. 324)
Anterior abdominal wall 1. Skin 2. Subcutaneous tissue 3. Superficial fascia of the abdomen 4. Fascia covering m. obliquus abdominis internus et transversus abdominis 5. M. transversus abdominis 6. F. transversalis 7. Parietal peritoneum spermatic cord and scrotum 1. Skin of the scrotum 2. Fleshy membrane of the scrotum (tunica dartos) 3. External seminal fascia (f. spermatica externa) 4. F. cremasterica 5. M. cremaster 6. Internal seminal fascia (f. spermatica interna) 7. Vaginal membrane ( tunica vaginalis testis on the testicle has: lamina perietalis, lamina visceralis)seminal vesicles
The seminal vesicle (vesicula seminalis) is a paired cellular organ up to 5 cm long, located lateral to the ampulla of the vas deferens. Above and in front it is in contact with the bottom of the bladder, behind - with the anterior wall of the rectum. Through it, seminal vesicles can be palpated. The seminal vesicle communicates with the terminal part of the vas deferens.
Function. Seminal vesicles do not live up to their name, as there are no spermatozoa in their secretion. By value, they are excretory glands that produce an alkaline reaction fluid that is ejected into the prostatic urethra at the time of ejaculation. The liquid mixes with the secretion of the prostate gland and a suspension of immobile spermatozoa coming from the ampulla of the vas deferens. Only in an alkaline environment do spermatozoa acquire mobility.
Age features. In a newborn, seminal vesicles look like twisted tubes, are very small and grow vigorously during puberty. They reach their maximum development by the age of 40. Then come involutive changes, primarily in the mucous membrane. In this regard, it becomes thinner, which leads to a decrease in secretory function.
ejaculatory duct
From the junction of the ducts of the seminal vesicles and the vas deferens, the ejaculatory duct (ductus ejaculatorius) 2 cm long begins, which passes through the prostate gland. The ejaculatory duct opens on the seminal tubercle of the prostatic urethra.
Prostate
The prostate gland (prostata) is an unpaired glandular-muscular organ that has the shape of a chestnut. It is located under the bottom of the bladder on the urogenital diaphragm of the pelvis behind the symphysis. It has a length of 2-4 cm, a width of 3-5 cm, a thickness of 1.5-2.5 cm and a weight of 15-25 g. It is possible to palpate the gland only through the rectum. The urethra and ejaculatory canals pass through the gland. In the gland, a base (basis) is distinguished, facing the bottom of the bladder (Fig. 329). and the apex (apex) - to the urogenital diaphragm. On the back surface of the gland, a groove is felt, which divides it into the right and left lobes (lobi dexter et sinister). The part of the gland located between the urethra and the ejaculatory duct stands out as the middle lobe (lobus medius). The anterior lobe (lobus anterior) is located in front of the urethra. Outside, it is covered with a dense connective tissue capsule. Vascular plexuses lie on the surface of the capsule and in its thickness. The connective tissue fibers of its stroma are woven into the capsule of the gland. From the anterior and lateral surfaces of the prostate capsule, the middle and lateral (paired) ligaments (lig. puboprostaticum medium, ligg. puboprostatica lateralia) begin, which are attached to the pubic fusion and to the anterior part of the tendon arch of the pelvic fascia. Among the ligaments there are muscle fibers, which are distinguished by a number of authors into independent muscles (m. puboprostaticus).
The parenchyma of the gland is divided into lobes and consists of numerous external and periurethral glands. Each gland opens with its own duct into the prostate urethra. The glands are surrounded by smooth muscle and connective tissue fibers. At the base of the gland, surrounding the urethra, there are smooth muscles, anatomically and functionally combined with the internal sphincter of the canal. In old age, hypertrophy of the periurethral glands develops, which causes narrowing of the prostatic urethra.
Function. The prostate gland produces not only an alkaline secretion for the formation of sperm, but also hormones that enter the sperm and blood. The hormone stimulates the spermatogenic function of the testicles.
Age features. Before puberty, the prostate gland, although it has the beginnings of a glandular part, is a muscular-elastic organ. During puberty, iron increases 10 times. It reaches its highest functional activity at the age of 30-45, then there is a gradual fading of the function. In old age, due to the appearance of collagen connective tissue fibers and atrophy of the glandular parenchyma, the organ thickens and hypertrophies.
prostate uterus
The prostatic uterus (utriculus prostaticus) has the shape of a pocket, which is located in the seminal tubercle of the prostatic part of the urethra. It is not related to the prostate gland in origin and is a remnant of the urinary ducts.
External male genital organs
male penis
The penis (penis) is a combination of two cavernous bodies (corpora cavernosa penis) and one spongy body (corpus spongiosum penis), covered on the outside with membranes, fascia and skin.
When viewed from the penis, the head (glans), body (corpus) and root (radix penis) are isolated. On the head there is a vertical slot of the external opening of the urethra with a diameter of 8-10 mm. The surface of the penis, facing upward, is called the back (dorsum), the lower one is the urethra (facies urethralis) (Fig. 326).

The skin of the penis is thin, delicate, mobile and devoid of hair. In the anterior part, the skin forms a fold of the foreskin (preputium), which in children tightly covers the entire head. According to the religious rites of some peoples, this fold is removed (the rite of circumcision). On the underside of the head there is a frenulum (frenulum preputii), from which the suture begins along the midline of the penis. Around the head and on the inner sheet of the foreskin there are many sebaceous glands, the secret of which is secreted into the groove between the head and the fold of the foreskin. There are no mucous and sebaceous glands on the head, and the epithelial lining is thin and delicate.
Cavernous bodies (corpora cavernosa penis), paired, (Fig. 327) are built from fibrous connective tissue, which has a cellular structure of transformed blood capillaries, so it resembles a sponge. With the contraction of the muscle sphincters of venules and m. ischiocavernosus, which compresses v. dorsalis penis, the outflow of blood from the chambers of the cavernous tissue is difficult. Under the pressure of blood, the chambers of the cavernous bodies straighten out and an erection of the penis occurs. The anterior and posterior ends of the cavernous bodies are pointed. At the front end, they are fused with the head (glans penis), and at the back in the form of legs (crura penis) grow to the lower branches of the pubic bones. Both cavernous bodies are enclosed in a protein shell (tunica albuginea corporum cavernosorum penis), which protects the chamber of the cavernous part from rupture during erection.

The spongy body (corpus spongiosum penis) is also covered with a protein membrane (tunica albuginea corporum spongiosorum penis). The anterior and posterior ends of the spongy body are expanded and form the head of the penis in front, and the bulb (bulbus penis) in the back. The spongy body is located on the lower surface of the penis in the groove between the cavernous bodies. The spongy body is formed by fibrous tissue, which also contains cavernous tissue, which is filled with blood during erection, like the cavernous bodies. In the thickness of the spongy body passes the urethra for the excretion of urine and sperm.
Cavernous and spongy bodies, with the exception of the head, are surrounded by deep fascia (f. penis profunda), which is covered with superficial fascia. Between the fascia are blood vessels and nerves (Fig. 328).

Age features. The penis grows vigorously only during puberty. In the elderly, there is a greater keratinization of the epithelium of the head, foreskin and skin atrophy.
Erection and sperm ejaculation
For fertilization, one sperm is needed, which connects with the egg in the fallopian tube or peritoneal cavity of the woman. This is achieved when the spermatozoa enter the female genital tract. When filling the vascular system of the penis, an erection is possible. When the glans penis is rubbed against the vagina, the labia minora and labia majora, with the participation of the spinal centers, a reflex contraction of the muscle elements of the ampulla of the vas deferens, seminal vesicles, prostate and cooper glands occurs. Their secret, mixed with spermatozoa, is thrown into the urethra. In the alkaline environment of the secretion of the prostate gland, spermatozoa acquire mobility. With the contraction of the muscles of the urethra and perineum, the sperm is poured into the vagina.
male urethra
The male urethra (urethra masculina) is about 18 cm long; most of it mainly passes through the spongy body of the penis (Fig. 329). The canal begins in the bladder with an internal opening and ends with an external opening on the glans penis. The urethra is divided into prostatic (pars prostatica), membranous (pars membranacea) and spongy (pars spongiosa) parts.
The prostate corresponds to the length of the prostate and is lined with transitional epithelium. In this part, a narrowed place is distinguished according to the position of the internal sphincter of the urethra and below an expanded part 12 mm long. On the back wall of the expanded part is the seminal tubercle (folliculus seminalis), from which the scallop (crista urethralis), formed by the mucous membrane, extends up and down. Around the mouths of the ejaculatory ducts, which open on the seminal tubercle, there is a sphincter. In the tissue of the ejaculatory ducts there is a venous plexus, which acts as an elastic sphincter.
The membranous part represents the shortest and narrowest section of the urethra; it is well fixed in the urogenital diaphragm of the pelvis and has a length of 18-20 mm. Striated muscle fibers around the canal form an external sphincter (sphincter urethralis externus), subordinate to the human mind. The sphincter, except for the act of urination, is constantly reduced.
The spongy part has a length of 12-14 cm and corresponds to the spongy body of the penis. It begins with a bulbous expansion (bulbus urethrae), where the ducts of two bulbous urethra glands open, secreting protein mucus to moisten the mucous membrane and thin the sperm. Bulbourethral glands the size of a pea are located in the thickness of m. transversus perinei profundus. The urethra of this part starts from the bulbous expansion, has a uniform diameter of 7-9 mm, and only in the head passes into a spindle-shaped expansion called the navicular fossa (fossa navicularis), which ends with a narrowed external opening (orificium urethrae externum). In the mucous membrane of all sections of the canal, there are numerous glands of two types: intraepithelial and alveolar-tubular. The intraepithelial glands are similar in structure to goblet mucous cells, and the alveolar-tubular glands are flask-shaped, lined with a cylindrical epithelium. These glands secrete a secret to moisten the mucous membrane. The basement membrane of the mucosa is fused with the spongy layer only in the spongy part of the urethra, and in other parts - with the smooth muscle layer.
When considering the profile of the urethra, two curvatures, three expansions and three narrowings are distinguished. The anterior curvature is located in the root area and is easily corrected by lifting the penis. The second curvature is fixed in the perineum and goes around the pubic fusion. Canal extensions: in the pars prostatica - 11 mm, in the bulbus urethrae - 17 mm, in the fossa navicularis - 10 mm. Narrowing of the channel: in the area of the internal and external sphincters, the channel is completely closed, in the area of \u200b\u200bthe external opening, the diameter decreases to 6-7 mm. Due to the extensibility of the canal tissue, if necessary, it is possible to pass a catheter with a diameter of up to 10 mm.
urethrograms
With ascending urethrography, the cavernous part of the male urethra has a shadow in the form of an even strip; an expansion is noted in the bulbous part, the membranous part is narrowed, the prostate is expanded. The membranous and prostatic parts make up the posterior urethra, located at right angles to its two anterior parts.
Scrotum
The scrotum (scrotum) is formed by skin, fascia and muscle; it contains the spermatic cords and testicles. The scrotum is located in the perineum between the root of the penis and the anus. The layers of the scrotum are discussed in the "Spermoid cord" section.
The skin of the scrotum is richly pigmented, thin, on its surface in young people there are transverse folds, which, when the muscle membrane contracts, constantly change their depth and shape. In the elderly, the scrotum sags, the skin becomes thinner, loses folding. The skin has sparse hair, many sebaceous and sweat glands. In the midline, there is a middle suture (raphe scroti), devoid of pigment, hair and glands, and in the depths of the scrotum there is a septum (septum scroti). The skin is adjacent to the fleshy membrane (tunica dartos) and therefore is devoid of subcutaneous tissue.
Female reproductive organs
The female genital organs (organa genitalia feminina) are conditionally divided into internal - ovaries, uterus with tubes, vagina and external - genital gap, hymen, large and small labia and clitoris.
Internal female reproductive organs
Ovary
The ovary (ovarium) is a paired female gonad, having an oval shape, length 25 mm, width 17 mm, thickness 11 mm, weight 5-8 g. The ovary is located vertically in the cavity of the small pelvis. Distinguish between its tubal end (extremitas tubaria) and uterine end (extremitas uterina), medial and lateral surfaces (facies medialis et lateralis), free posterior (margo liber) and mesenteric (margo mesovaricus) edges.
The ovary is located on the lateral surface of the small pelvis (Fig. 280) in a hole bounded from above a. et v. iliacae externae, below - aa. uterina et umbilicalis, in front - by the parietal peritoneum when it passes into the posterior leaf of the broad ligament of the uterus, behind - a. et v. iliacae externae. The ovary lies in this fossa in such a way that the tubal end is directed upward, the uterine end is downward, the free edge is directed backward, the mesenteric is forward, the lateral surface is adjacent to the parietal peritoneum of the pelvis, and the medial one is turned towards the uterus.
In addition to the mesentery (mesosalpinx), the ovary is fixed to the side wall of the pelvis with two ligaments. Suspension ligament (lig. suspensorium ovarii) starts from the tubular end of the ovary and ends in the parietal peritoneum at the level of the renal veins. Arteries and veins, nerves and lymphatic vessels pass through this ligament to the ovary. Own ligament of the ovary (lig. ovarii proprium) goes from the uterine end to the lateral corner of the uterine fundus.
The parenchyma of the ovary contains follicles (folliculi ovarici vesiculosi), (Fig. 330), which contain developing eggs. Primary follicles are located in the outer layer of the cortical substance of the ovary, which gradually move into the depth of the cortical substance, turning into a vesicular follicle. Simultaneously with the development of the follicle, an egg (oocyte) develops.

Blood and lymphatic vessels, thin connective tissue fibers and small strands of invaginated enzymatic epithelium, surrounded by follicular epithelium, pass between the follicles. These follicles lie in a continuous layer under the epithelium and albuginea. Every 28 days, usually one follicle develops, having a diameter of 2 mm. With its proteolytic enzymes, it melts the protein membrane of the ovary and, bursting, releases the egg. The ovum released from the follicle enters the peritoneal cavity, where it is captured by the fimbriae of the fallopian tube. In place of the bursting follicle, a corpus luteum (corpus luteum) is formed that produces lutein, and then progesterone, which inhibits the development of new follicles. In the case of conception, the corpus luteum develops rapidly and, under the action of the lutein hormone, inhibits the maturation of new follicles. If pregnancy does not occur, under the influence of estradiol, the corpus luteum atrophies and overgrows with a connective tissue scar. After atrophy of the corpus luteum, new follicles begin to mature. The mechanism that regulates the maturation of follicles is under the control of not only hormones, but also the nervous system.
Function. The ovary is not only an organ for the maturation of the egg, but also an endocrine gland. The development of secondary sexual characteristics and the psychological characteristics of the female body depend on the hormones that enter the bloodstream. These hormones are estradiol, produced by follicular cells, and progesterone, produced by corpus luteum cells. Estradiol promotes the maturation of follicles and the development of the menstrual cycle, progesterone ensures the development of the embryo. Progesterone also enhances the secretion of the glands and the development of the uterine mucosa, reduces the excitability of its muscle elements, and stimulates the development of the mammary glands.
Age features. The ovaries in newborns are very small 0.4 g and in the first year of life increase 3 times. Under the ovarian albuginea in newborns, the follicles are arranged in several rows. In the first year of life, the number of follicles decreases significantly. In the second year of life, the albuginea thickens and its bridges, plunging into the cortical substance, separate the follicles into groups. By the period of puberty, the ovary has a mass of 2 g. At 11-15 years old, intensive maturation of the follicles, their ovulation and menstruation begin. The final formation of the ovary is observed by the age of 20.
After 35-40 years, the ovaries slightly decrease. After 50 years, the menopause begins, the mass of the ovaries decreases by 2 times due to fibrosis and atrophy of the follicles. The ovaries turn into dense connective tissue formations.
Ovarian appendages
Ovarian appendages (epoophoron and paroophoron) are a paired rudimentary formation representing the remnants of mesonephros. It is located between the sheets of the broad ligament of the uterus in the mesosalpinx region.
Uterus
The uterus (uterus) is an unpaired, pear-shaped hollow organ. It distinguishes the bottom (fundus uteri), body (corpus), isthmus (isthmus) and neck (cervix) (Fig. 330). The bottom of the uterus is the highest part, protruding above the mouths of the fallopian tubes. The body is flattened and gradually narrows to the isthmus. The isthmus is the most narrowed part of the uterus, 1 cm long. The cervix has a cylindrical shape, starts from the isthmus and ends in the vagina with the anterior and posterior lips (labia anterius et posterius). The posterior lip is thinner and protrudes more into the lumen of the vagina. The uterine cavity has an irregular triangular fissure. In the region of the bottom of the uterus, there is the base of the cavity, into which the mouths of the fallopian tubes (ostium uteri) open, the top of the cavity passes into the cervical canal (canalis cervicis uteri). In the cervical canal, internal and external openings are distinguished. In nulliparous women, the external opening of the cervix has an annular shape, in those who have given birth, it has the shape of a gap, which is due to its ruptures during childbirth (Fig. 331).

The length of the uterus is 5-7 cm, the width in the bottom area is 4 cm, the wall thickness reaches 2-2.5 cm, the weight is 50 g. -4 ml of liquid, in those giving birth - 5-7 ml. The diameter of the cavity of the uterine body is 2-2.5 cm, in those who gave birth - 3-3.5 cm, the neck has a length of 2.5 cm, in those who gave birth - 3 cm, the diameter is 2 mm, in those who gave birth - 4 mm. Three layers are distinguished in the uterus: mucous, muscular and serous.
The mucous membrane (tunica mucosa seu, endometrium) is lined with ciliated epithelium, penetrated by a large number of simple tubular glands (gll. uterinae). In the neck there are mucous glands (gll. cervicales). The thickness of the mucous membrane ranges from 1.5 to 8 mm, depending on the period of the menstrual cycle. The mucous membrane of the body of the uterus continues into the mucous membrane of the fallopian tubes and cervix, where it forms palm-like folds (plicae palmatae). These folds are clearly expressed in children and nulliparous women.
The muscular coat (tunica muscularis seu, myometrium) is the thickest layer formed by smooth muscles interspersed with elastic and collagen fibers. It is impossible to isolate individual muscle layers in the uterus. Studies show that in the process of development, when the two urinary canals merged, the circular muscle fibers intertwined with each other (Fig. 332). In addition to these fibers, there are circular fibers braiding corkscrew-shaped arteries, oriented radially from the surface of the uterus to its cavity. In the region of the neck, the loops of muscle spirals have a sharp bend and form a circular muscle layer.

The serous membrane (tunica serosa seu, perimetrium) is represented by the visceral peritoneum, which is firmly adherent to the muscular membrane. The peritoneum of the anterior and posterior walls along the edges of the uterus is connected into wide uterine ligaments, below, at the level of the isthmus, the peritoneum of the anterior wall of the uterus passes to the posterior wall of the bladder. A deepening (excavatio vesicouterina) is formed at the transition point. The peritoneum of the posterior wall of the uterus completely covers the cervix and is even fused for 1.5-2 cm with the posterior wall of the vagina, then passes to the anterior surface of the rectum. Naturally, this depression (excavatio rectouterina) is deeper than the vesicouterine cavity. Due to the anatomical connection of the peritoneum and the posterior wall of the vagina, diagnostic punctures of the recto-uterine cavity are possible. The peritoneum of the uterus is covered with mesothelium, has a basement membrane and four connective tissue layers oriented in different directions.
Bundles. The broad ligament of the uterus (lig. Latum uteri) is located along the edges of the uterus and, being in the frontal plane, reaches the side wall of the small pelvis. This ligament does not stabilize the position of the uterus, but performs the function of the mesentery. In conjunction, the following parts are distinguished. 1. The mesentery of the fallopian tube (mesosalpinx) is located between the fallopian tube, the ovary and its own ligament of the ovary; between the leaves of mesosalpinx are epoophoron and paroophoron, which are two rudimentary formations. 2. The fold of the posterior peritoneum of the broad ligament forms the mesentery of the ovary (mesovarium). 3. The part of the ligament located below the proper ligament of the ovary constitutes the mesentery of the uterus, where loose connective tissue (parametrium) lies between its sheets and on the sides of the uterus. Through the entire mesentery of the broad ligament of the uterus, vessels and nerves pass to the organs.
The round ligament of the uterus (lig. teres uteri) is steam room, has a length of 12-14 cm, a thickness of 3-5 mm, starts at the level of the orifices of the fallopian tubes from the anterior wall of the body of the uterus and passes between the leaves of the broad uterine ligament down and laterally. Then it penetrates into the inguinal canal and ends on the pubis in the thickness of the labia majora.
The main ligament of the uterus (lig. cardinale uteri) is a steam room, located in the frontal plane at the base of the lig. latum uteri. It starts from the cervix and attaches to the lateral surface of the pelvis, fixes the cervix.
The recto-uterine and vesico-uterine ligaments (Hgg. rectouterina et vesicouterina), respectively, connect the uterus to the rectum and bladder. The ligaments contain smooth muscle fibers.
Topography and position of the uterus. The uterus is located in the pelvic cavity between the bladder in front and the rectum in the back. Palpation of the uterus is possible through the vagina and rectum. The bottom and body of the uterus are mobile in the small pelvis, so the filled bladder or rectum affects the position of the uterus. With empty pelvic organs, the bottom of the uterus is directed forward (anteversio uteri). Normally, the uterus is not only tilted forward, but also bent in the isthmus (anteflexio). The opposite position of the uterus (retroflexio), as a rule, is considered pathological.
Function. The fetus is born in the uterine cavity. During childbirth, the fetus and placenta are expelled from the uterine cavity by contraction of the muscles of the uterus. In the absence of pregnancy, rejection of the hypertrophied mucous membrane occurs during the menstrual cycle.
Age features. The uterus of a newborn girl has a cylindrical shape, a length of 25-35 mm and a mass of 2 g. The cervix is 2 times longer than her body. There is a mucous plug in the cervical canal. Due to the small size of the small pelvis, the uterus is located high in the abdominal cavity, reaching the fifth lumbar vertebra. The anterior surface of the uterus is in contact with the posterior wall of the bladder, the posterior wall is in contact with the rectum. The right and left edges are in contact with the ureters. After birth during the first 3-4 weeks. the uterus grows faster and a well-defined anterior curve is formed, which is then preserved in an adult woman. By the age of 7, the bottom of the uterus appears. The size and weight of the uterus are more constant up to 9-10 years. Only after 10 years does the rapid growth of the uterus begin. Its weight depends on age and pregnancies. At 20 years old, the uterus weighs 23 g, at 30 years old - 46 g, at 50 years old - 50 g.
The fallopian tubes
The fallopian tube (tuba uterina) is a paired oviduct through which the egg moves from the peritoneal cavity after ovulation to the uterine cavity. The fallopian tube is divided into the following parts: pars uterina - passes through the wall of the uterus, isthmus - the narrowed part of the tube, ampulla - expansion of the tube, infundibulum - the end part of the tube, representing the shape of a funnel bordered by fringes (fimbriae tubae) and located on the side wall of the pelvis near the ovary . The last three parts of the tube are covered with peritoneum and have a mesentery (mesosalpinx). Pipe length 12-20 cm; its wall contains mucous, muscular and serous membranes.
The mucous membrane of the tube is covered with stratified ciliated prismatic epithelium, which contributes to the promotion of the egg. In fact, the lumen of the fallopian tube is absent, since it is filled with longitudinal folds with additional villi (Fig. 333). With minor inflammatory processes, part of the folds can grow together with each other, being an insurmountable obstacle to the advancement of a fertilized egg. In this case, an ectopic pregnancy may develop, since the narrowing of the fallopian tube is not an obstacle to the sperm. Obstruction of the fallopian tubes is one of the causes of infertility.

The muscular coat is represented by the outer longitudinal and inner circular layers of smooth muscles, which directly continue into the muscular coat of the uterus. Peristaltic and pendulum contractions of the muscle layer contribute to the movement of the egg into the uterine cavity.
The serous membrane represents the visceral peritoneum, which closes below and passes into the mesosalpinx. Under the serous membrane there is a loose connective tissue.
Topography. The fallopian tube is located in the small pelvis in the frontal plane. It follows almost horizontally from the angle of the uterus, and in the region of the ampulla forms a curve backwards with a bulge upwards. The funnel of the tube descends parallel to the margo liber of the ovary.
Age features. In newborns, the fallopian tubes are tortuous and relatively longer, so they form several bends. By the time of puberty, the tube straightens out, keeping one bend. In older women, the bends of the tube are absent, its wall becomes thinner, the fringes atrophy.
X-rays of the uterus and tubes (hysterosalpingograms)
The shadow of the uterine cavity has a triangular shape (Fig. 334). If the fallopian tubes are passable, then the intra-wall narrowed part of the tube begins from the base of the triangle, then it, expanding in the isthmus, passes into the ampoule. The contrast agent enters the peritoneal cavity. On the pictures of the uterus, it is possible to establish the deformation of the uterine cavity, the patency of the tubes, the presence of a bicornuate uterus, etc.

Menstrual cycle
Unlike the male activity of the female reproductive system, it proceeds cyclically with a frequency of 28-30 days. The cycle ends with the onset of menstruation. The menstrual period is divided into three phases: menstrual, postmenstrual and premenstrual. In each phase, the structure of the mucous membrane has its own characteristics depending on the function of the ovaries (Fig. 335).

1. The menstrual phase lasts 3-5 days. During this period, the mucous membrane, as a result of spasm and rupture of blood vessels, is torn away from the basal layer. Only parts of the uterine glands and small islands of the epithelium remain in it. In the menstrual phase, 30-50 ml of blood flows out.
2. In the postmenstrual (intermediate) phase, the process of restoration of the mucous membrane occurs under the influence of estrogen in the developing follicle. This phase lasts 12-14 days. Despite the fact that the uterine glands completely regenerate, their lumens remain narrow and, most importantly, devoid of secretion. After the 14th day, ovulation of the egg occurs and the formation of a corpus luteum that secretes progesterone, which is a powerful stimulant for the development of the glands of the mucous membrane and uterine epithelium.
3. The premenstrual (functional) phase lasts 10 days. During this time, under the action of progesterone, the glands of the uterine mucosa secrete a secret, glycogen and lipid granules, vitamins and microelements accumulate in epithelial cells. If fertilization occurs, then the embryo is introduced onto the prepared mucous membrane with the subsequent development of the placenta. In the absence of fertilization of the egg, menstruation occurs - rejection of the mucous membrane and hypertrophied mucous glands.
Vagina
The vagina (vagina) is an easily stretchable muco-muscular tube 3 mm thick and up to 10 cm long. The vagina starts from the cervix and opens into the genital slit with a hole. Its anterior and posterior walls (parietes anterior et posterior) are in contact with each other. At the place of attachment of the vagina to the cervix, there are anterior and posterior arches (fornices anterior et posterior). The posterior fornix is deeper and contains vaginal fluid. This is where sperm is poured during copulation. The opening of the vagina (ostium vaginae) is covered by the hymen (hymen).
The hymen is a derivative of the Mullerian tubercle, which appears at the end of the vagina at the confluence of the urinary ducts. The mesenchyme of the Müllerian tubercle grows and covers the urogenital sinus with a thin plate. Only for the 6th month of embryonic development, holes appear in the plate. The hymen is a semilunar or perforated plate with a hole of about 1.5 cm. During intercourse or childbirth, the hymen is torn and its remnants atrophy, forming shreds (carunculae hymenales).
The vaginal wall is made up of three layers. The mucous membrane is covered with stratified squamous epithelium, tightly fused with a hypertrophied basement membrane, which is connected to the muscular membrane. This protects the mucous membrane from damage during intercourse and childbirth. In nulliparous women, the vaginal mucosa has distinct transverse wrinkles (rugae vaginales), as well as longitudinal folds in the form of columns of wrinkles (columnae rugarum), among which there are anterior and posterior columns (columnae rugarum anterior et posterior). After childbirth, the mucous membrane of the vagina, as a rule, becomes smooth. Mucous glands were not found in it, and the acidic secret of the vagina is a waste product of microorganisms that destroy glycogen granules, exfoliating epithelial cells. As a result of this mechanism, a biological protective barrier is formed for many microorganisms that are inactive in the acidic environment of the vagina. Alkaline sperm and the secretion of the glands of the vestibule partially neutralize the acidic environment of the vagina, ensuring sperm motility.
The muscular coat has a reticulate structure due to the mutual interlacing of spiral smooth muscle bundles. Striated muscle fibers around the opening of the vagina form a muscle pulp (sphincter urethrovaginalis) 5-7 mm wide, which also covers the urethra.
The connective sheath (tunica adventitia) consists of loose connective tissue in which the vascular and nerve plexuses lie.
Topography. Most of the vagina lies on the urogenital diaphragm. The anterior wall of the vagina is fused with the urethra, the posterior - with the anterior wall of the rectum. On the sides and in front from the outside, at the level of the arches, the vagina is in contact with the ureters. The final part of the vagina is connected with the muscles and fascia of the perineum, which take part in strengthening the vagina.
Age features. The vagina of a newborn girl has a length of 23-35 mm and an obliterated lumen. The anterior wall is in contact with the urethra, the posterior - with the rectum. Only during the period of increase in the size of the pelvis, when the bladder descends, does the position of the anterior fornix of the vagina change. At 10 months the internal opening of the urethra is at the level of the anterior fornix of the vagina. At 15 months the level of the arch corresponds to the triangle of the bladder. After 10 years, increased growth of the vagina and the formation of mucosal folds begin. At 12-14 years old, the anterior fornix is located above the entry of the ureters.
Function. The vagina serves for copulation, being a reservoir for sperm. The fetus is expelled through the vagina. Irritation of the nerve receptors of the vagina during intercourse causes sexual arousal (orgasm).
External female genital organs (Fig. 336)

Large labia
Large labia (labia majora pudendi) are located in the perineum and are paired skin rollers 8 cm long, 2-3 cm thick. Both lips limit the genital gap (rima pudendi). The right and left lips are joined in front and behind by adhesions (commissurae labiorum anterior et posterior). The labia majora, with the exception of the medial surface, are covered with sparse hair and are richly pigmented. The medial surface faces the genital fissure and is lined with a thin layer of stratified squamous epithelium.
Small labia
The labia minora (labia minora pudendi) is located in the genital gap medial to the labia majora. They represent thin paired skin folds, as a rule, not visible in a closed genital fissure. Rarely, the labia minora are higher than the large ones. In front, the labia minora go around the clitoris and form the foreskin (preputium clitoridis), which fuses under the head of the clitoris into a frenulum (frenulum clitoridis), and also forms a transverse frenulum (frenulum labiorum pudendi) from behind. The labia minora is covered with a thin layer of stratified squamous epithelium. They are based on loose connective tissue with vascular and nerve plexuses.
Vaginal vestibule
The vestibule of the vagina (vestibulum vaginae) is limited by the medial surfaces of the labia minora, in front - by the frenulum of the clitoris, behind - by the frenulum of the labia minora, from the outside it opens into the genital gap.
In the vestibule, the ducts of the paired large glands of the vestibule (gll. vestibulares majores) open. These pea-sized glands are located at the base of the labia majora in the thickness of the deep transverse perineal muscle and, therefore, are similar to the male bulbo-urethral glands. A duct 1.5 cm long opens on the medial surface at the base of the labia minora 1-2 cm anterior to its transverse frenulum. The secret of the large glands of the vestibule of white color, alkaline reaction, is released during the contraction of the muscles of the perineum and moisturizes the genital slit and the vestibule of the vagina.
In addition to the paired large glands of the vestibule, there are small glands (gll. vestibulares minores), which open between the opening of the urethra and the vagina.
Clitoris
The clitoris (clitoris) is formed by two cavernous bodies (corpora cavernosa clitoridis). It has a head, body and legs. The body is 2-4 cm long and is covered with dense fascia (f. clitoridis). The head lies in the upper part of the genital slit, has a frenulum (frenulum clitoridis) from below, and the foreskin (preputium clitoridis) from above. The legs are attached to the lower branches of the pubic bones. Thus, the clitoris in structure resembles the penis, only devoid of a spongy body, and is smaller.
Function. With sexual arousal, the clitoris lengthens and becomes elastic. The clitoris is richly innervated and contains numerous sensitive endings; there are especially many genital bodies in it, which perceive irritations that occur during sexual intercourse.
Bulb vestibule
Bulb vestibule (bulbus vestibuli) in origin corresponds to the spongy body of the penis. The difference is that the spongy tissue in a woman is divided into two parts by the urethra and is located around not only this channel, but also the vestibule of the vagina.
Function. When excited, the spongy tissue swells and narrows the entrance to the vestibule of the vagina. After orgasm, the blood from the vestibular bulb chambers drains and the swelling subsides. The bulb of the vestibule is especially developed in some monkeys.
Age features of the external female genital organs. In a newborn girl, the clitoris and labia minora protrude from the genital slit. By the age of 7-10, the genital gap opens only when the hips are divorced. During childbirth, the vestibule of the vagina, the frenulum and adhesions of the labia are sometimes torn; the vagina is stretched, many folds of its mucous membrane are smoothed out. In conditions where the vaginal vestibule is stretched, the genital slit is open. In this case, protrusion of the anterior or posterior wall of the vagina is possible. After 45-50 years, atrophy of the labia, large and small mucous glands of the vestibule occurs, thinning and keratization of the mucous membrane of the genital slit and vagina are noted.
Crotch
The perineum (perineum) represents all soft formations (skin, muscles, fascia) located at the exit of the small pelvis, limited in front by the pubic bones, behind by the coccyx, and laterally ischial tubercles. Due to the large size of the small pelvis in women and the perineum is slightly larger than in men. In women, the perineum is clearly visible with the hips apart. In men, the perineum is not only narrower, but also deeper. The perineum can be divided by the intersciatic line passing between the ischial tubercles into the anterior (genitourinary) and posterior (anal) regions. The urogenital region is strengthened by the urogenital diaphragm (diaphragma urogenitale), through which the urethra passes, and in women, the vagina. The anal region contains the pelvic diaphragm (diaphragma pelvis), through which only the rectum passes.
The perineum is covered with pigmented thin skin, contains sebaceous, sweat glands and sparse hair. Subcutaneous fat and fascia are unevenly developed. The urogenital and pelvic diaphragms withstand the weight of the internal organs and intra-abdominal pressure, preventing the internal organs from falling into the perineum. In addition, the muscles of the perineum form arbitrary sphincters of the urethra and rectum.
Urogenital diaphragm (Fig. 337, 338)


The urogenital diaphragm (diaphragma urogenitale) consists of striated muscles.
1. The bulbous-spongy muscle (m. bulbospongiosus) is steam room, in men it is located on the corpus spongiosum bulb. It starts on the lateral surface of the cavernous bodies and, meeting with the muscle of the same name of the opposite side along the midline of the spongy body, forms a suture.
Function. Muscle contraction promotes the ejection of sperm and urination.
In women m. bulbospongiosus covers the opening of the vagina (see Fig. 339). In those who have given birth, this muscle, as a rule, is torn and atrophied, as a result of which the entrance to the vagina is more open than in those who have not given birth.
2. Ischiocavernosus muscle (m. ischiocavernosus) steam room, starts from the ischial tubercles and the anterior branch of the ischium and ends on the fascia of the cavernous body.
Function. The muscle contributes to the erection of the penis or clitoris. When the muscle contracts, the fascia of the root of the penis or clitoris tenses and compresses v. dorsalis penis or v. clitoridis, preventing the outflow of blood from the penis or clitoris.
3. Superficial transverse muscle of the perineum (m. transversus perinei superficialis) paired, weak, located behind m. bulbospongiosus, starting from the ischial tuberosity; ends in the center of the perineum.
4. Deep transverse muscle (m. transversus perinei profundus) steam room, starts from the lower branch of the pubic bone and ends in the median tendon suture. In its thickness lie gl. bulbourethralis (in men) and gl. vestibularis major (in women).
Function. Strengthens the urogenital diaphragm.
5. The external sphincter of the urethra (m. sphincter urethrae externus) surrounds its membranous part. The muscle is represented by annular bundles - derivatives of m. transversus perinei profundus. In women, the sphincter is less developed.
pelvic diaphragm
The pelvic diaphragm (diaphragma pelvis) also includes muscles.
1. External sphincter of the anus (m. sphincter ani externus), circularly covers the anus, located under the skin (Fig. 339).

Function. It is under the control of human consciousness. Closes anus.
2. The muscle that lifts the anus (m. levator ani), steam room, triangular shape. It starts on the lateral surface of the small pelvis from the lower branch of the pubic bone (pars pubica m. pubococcygei), from the tendon arch of the obturator fascia (pars iliaca m. iliococcygei), covering the internal obturator muscle; descending to the anus, the bundles converge.
Function. It is determined depending on the beginning of the muscle bundles. The bundles of the pubic part of the muscle, contracting, press the anterior wall of the intestine to the posterior. When the ampulla of the rectum is full, the pubic part of the anus lift promotes defecation, and when the ampulla of the rectum is empty, it closes. In women, the pubic part m. levator ani compresses the vagina. The second part m. levator ani, iliac, raises the anus. In general, both parts of the muscle, having the shape of a funnel, open into the abdominal cavity and consisting of a thin muscle plate, withstand a relatively large pressure of the viscera. The strength of the muscle is due to the fact that, under intra-abdominal pressure, it is pressed against the walls of the pelvis, where in the center of this muscle funnel, the rectum is a "locking wedge".
3. The coccygeal muscle (m. coccygeus) in the form of a paired plate covers the bottom of the pelvis, starting from the IV-V sacral vertebrae and the coccyx, is attached to the sciatic spine and lig. sacrospinosum.
Fascia of the pelvis, perineum and interfascial tissue
Fascia of the pelvic diaphragm. The fascia of the pelvic diaphragm is anatomically related to the pelvic fascia (f. pelvis), which is a continuation of the iliac fascia located in the large pelvis. The pelvic fascia covers the back of the sacrum and piriformis muscles, laterally - internal obturator muscles and, reaching the tendon arc (arcus tendineus) of the pelvis, from which m. levator ani, is divided into parietal sheet (f. pelvis parietalis) and the upper fascia of the pelvic diaphragm (f. diaphrag-matis pelvis superior). The parietal sheet below the tendon arch covers the walls of the pelvis and ends on the ischial tuberosities, pubic bones, ischiosacral, sacrospinous ligaments. Ahead, it forms the ligaments of the prostate (see Prostate gland). The upper diaphragmatic sheet of the pelvic fascia lies on m. levator ani and m. coccygeus from above and is woven into the external sphincter of the rectum (m. sphincter ani externus). From the outer surface, i.e. from the side of the crotch, m. levator ani is lined with the lower fascia of the pelvic diaphragm (f. diaphragmatis pelvis). This fascia continues from the gluteus maximus muscle, then covers the ischial bones, partially - m. obturatorius internus and, moving to the lower surface of m. levator ani, ends in the external sphincter of the rectum (Fig. 340).

The subcutaneous tissue in the region of the pelvic diaphragm is covered with the superficial fascia of the perineum (f. perinei superficial), which is part of the subcutaneous fascia of the body. Thus, between the rectum, the side wall of the pelvis and, from below, the superficial fascia of the perineum, an ischiorectal fossa (fossa ischiorectalis) is formed, filled with fatty tissue. This fossa has the shape of a triangular pyramid, with the apex facing upwards. In men, it is much deeper than in women. In children, it has the shape of a narrow slit and is relatively deep.
Interfascial tissue of the pelvis. Between the peritoneum lining the small pelvis, and f. diaphragmatis pelvis space does not exist, but there is a layer of loose fatty tissue with many venous and nerve plexuses, which is located in front of the bladder, behind the rectum and around the vagina.
Fascia of the urogenital diaphragm. The urogenital diaphragm has superior and inferior fascial layers. The upper fascial sheet is woven into m. transversus perinei profundus and m. sphincter urethrae externus. In the lateral parts, these sheets are fused with the capsule of the prostate gland. The lower fascial sheet covers the deep transverse perineal muscle and the external sphincter of the urethra, then the cavernous and spongy bodies with m. ischiocavernosus et bulbospongiosus, and is woven into the external sphincter of the rectum from behind. In women, both fasciae are woven into the wall of the vagina. Near the front edge of m. transversus perinei profundus, the upper and lower fascial sheets are connected to the transverse ligament of the pelvis (lig. transversus pelvis), which is adjacent to the lig. arcuatum pubis. Between these ligaments pass a. et v. dorsalis penis, nerves of the penis, clitoris, vagina and bulbus vestibularis. On the back edge m. transversus perinei profundus, the upper and lower fascial sheets also close, forming a common thin connective tissue plate covered by m. transversus perinei superficialis.
The superficial fascia of the perineum (f. perinei superficialis) directly passes from the pelvic diaphragm to the urogenital diaphragm and covers mm. bulbospongiosus, ischiocavernosus et transversus perinei superficialis, i.e. superficial muscles of the perineum. This fascia continues into the superficial fascia of the penis, inner thighs, and pubis.
Development of male and female internal genital organs
Male and female internal genital organs, although they differ significantly in structure, nevertheless have common rudiments. In the initial stage of development, there are common cells that are sources of formation of the sex glands associated with the urinary and genital ducts (mesonephros duct) (Fig. 341). During the period of differentiation of the gonads, development reaches only one pair of ducts. During the formation of a male individual, convoluted and straight testicular tubules, the vas deferens, seminal vesicles develop from the genital duct, and the urinary duct is reduced and only the male uterus remains in the colliculus seminalis as a rudimentary formation. When a female is formed, development reaches the urinary duct, which is the source of the formation of the fallopian tube, uterus and vagina, and the genital duct, in turn, is reduced, also giving a rudiment in the form of epoophoron and paroophoron.

Testicular development. The formation of the testis is associated with the ducts of the genitourinary system. At the level of the middle kidney (mesonephros), under the mesothelium of the body, the rudiments of the testis are formed in the form of strands of the testis, which are a derivative of the endodermal cells of the yolk sac. The gonadal cells of the testis cords develop around the ducts of the mesonephros (genital duct). For the fourth month intrauterine development, the seminal cord disappears and the testicle is formed. In this testicle, each tubule of the mesonephros divides into 3-4 daughter tubules, which turn into convoluted tubules that form testicular lobules. The convoluted tubules join into a thin straight tubule. Strands of connective tissue penetrate between the convoluted tubules, forming the interstitial tissue of the testis. The enlarging testis retracts the parietal peritoneum; as a result, a fold is formed above the testicle (phrenic ligament) and a lower fold (inguinal ligament of the genital duct). The lower fold turns into a conductor of the testis (gubernaculum testis) and takes part in the descent of the testicle. In the inguinal region, at the site of attachment of the gubernaculum testis, a protrusion of the peritoneum (processus vaginalis) is formed, which grows together with the structures of the anterior abdominal wall (Fig. 342). In the future, this protrusion will participate in the formation of the scrotum. After the formation of a protrusion of the peritoneum, the anterior wall of the recess closes into the internal inguinal ring. Testicle for VII-VIII months. prenatal development passes through the inguinal canal and at the time of birth is in the scrotum lying behind the peritoneal outgrowth, to which the testicle grows from its outer surface. When moving the testicle from the abdominal cavity to the scrotum or the ovary to the small pelvis, it is not entirely correct to talk about its true lowering. In this case, it is not a sinking that occurs, but a mismatch in growth. The ligaments above and below the gonads lag behind the growth rate of the trunk and pelvis and remain in place. As a result, the pelvis and trunk increase, and the ligaments and glands "go down" towards the developing trunk.

Anomalies of development. A common developmental anomaly is a congenital inguinal hernia, when the inguinal canal is so wide that through it the internal organs exit into the scrotum. Along with this, there is a testicular retention in the abdominal cavity near the internal opening of the inguinal canal (cryptorchidism).
Ovarian development. In the area of the seed cord in the female, germ cells are scattered in the mesenchymal stroma. The connective tissue base and sheath develop poorly. In the mesenchyme of the ovary, the cortical and brain zones are differentiated. In the cortical zone, follicles are formed, which in a newborn girl under the influence of mother's hormones increase, and then atrophy after birth. Vessels grow into the medulla. In the embryonic period, the ovary is located above the entrance to the small pelvis. With an increase in the ovary for the IV month. development, the inguinal ligament of mesonephros bends and turns into a suspensory ligament of the ovary. From its lower end, the proper ligament of the ovary and the round ligament of the uterus are formed. The ovary will be located between the two ligaments in the pelvis (Fig. 343).

Anomalies of development. Sometimes there is an additional ovary. A more frequent anomaly is a change in the topography of the ovary: it can be located at the internal opening of the inguinal canal, in the inguinal canal, or in the thickness of the labia majora. In these cases, anomalies in the development of the external genital organs can also be observed.
Development of the uterus, fallopian tubes and vagina. The epididymis, vas deferens and seminal vesicles develop from the genital duct in the wall of which a muscular layer is formed.
The fallopian tubes, uterus and vagina are formed by the transformation of the urinary ducts. This duct for the III month. development between the ovary and the uterus turns into a fallopian tube with an extension at the upper end. The fallopian tube is also drawn into the pelvis by the descending ovary (Fig. 344).

The urinary ducts in the lower part are surrounded by mesenchymal cells and form an unpaired tube, which for the second month. separated by a roller. The upper part is overgrown with mesenchymal cells, thickens and forms the uterus, and the vagina develops from the lower part.
Development of the external genitalia
Male and female external genitalia develop from a common sexual eminence (Fig. 345, 346).


Male external genitalia arise from the sexual eminence, from which the penis is formed. Laterally and posteriorly, there are two urogenital folds that meet along the midline of the penis over the urinary trough. In this case, a spongy part of the penis is formed. A seam is formed at the place of fusion of the folds. Simultaneously with the formation of the spongy part, the epithelium of the skin covers the head (part of the spongy body) of the penis, transforming into the foreskin. The genital folds of the inguinal region increase when the processus vaginales of the peritoneum penetrate into them, and also fuse along the midline into the scrotum.
In women, the genital tubercle is transformed into the clitoris, and the genital folds into the labia minora. The urethral groove on the genital tubercle does not close and the spongy part develops independently around the vagina, not being connected with the cavernous bodies of the clitoris. The labia majora develop from the genital folds. In these folds there is only adipose tissue, while in their homologue - the scrotum - there are testicles.
secretory gonads
The seminal vesicles develop from the terminal part of the genital duct.
The prostate gland is formed from the epithelium of the urethra, from which individual glands are formed, about 50 in number, wrapped in mesenchyme.
Bulbo-urethral glands are formed from the epithelial outgrowths of the spongy part of the urethra.
The secret of all these glands is involved in the formation of sperm and stimulation of sperm motility.
Alveolar-tubular glands of the urethra that secrete mucin develop from the epithelium of the urethra.
The large vestibular glands of a woman are a derivative of the epithelium of the urogenital sinus.
Anomalies of the external genitalia
The sex of a person is determined not by the external genital organs, but by the gonads. Due to the fact that the external genital organs develop from the genital tubercle, paired genital and urogenital folds and independently of the internal genital organs, developmental anomalies are often encountered. True hermaphroditism (bisexuality) occurs when the testicle and ovary develop. This anomaly is very rare and, as a rule, both glands are defective in their structure and function. False hermaphroditism is more common (Fig. 347). With false female hermaphroditism, the ovaries are located in the labia majora, which in this case resemble the scrotum. The hypertrophied clitoris covers a narrow genital gap. There is also male false hermaphroditism, when the testicles will be located in the thickness of the labia majora (i.e., the split scrotum), and the external genital organs are represented by the genital slit and the atrezated vagina.
An even more common anomaly in men is hypospadias, when the urinary folds that form the urethra do not close along the length of the urinary trough all along or in a limited area. In newborns, hypospadias is often mistaken for the genital gap and, due to incorrect sex determination, the boy is brought up as a girl.
Phylogeny of the reproductive system
In lower animals (sponges, hydra), germ cells have no connection with any particular germ layer or organ. These cells differentiate early and can be found in any layer of the body. In more highly organized animals (worms, arthropods, lancelets), not only heterosexual sex cells already exist, but also ways of their excretion appear. Vertebrates have all the elements of the reproductive system, but differ in structure. So, for example, in amphibians, reptiles, birds, the urinary passages do not merge and two independent oviducts develop. This can also explain the presence of two queens in rodents, elephants, pigs and other animals. Thus, a comparison of embryogenesis and phylogenesis shows the ways of formation and formation of the reproductive system. The external genital organs have a different origin in different animals. The genital organs are more complex in males. In selahia, the male copulatory organ is the posterior transformed fin. In bony fish, amphibians, as a rule, there are no organs of copulation, with the exception of viviparous fish, in which the penis is also a fin inserted into the cloaca of the female. Male reptiles have two types of copulatory organs. In snakes and lizards, the subcutaneous sacs protrude through the cloaca to the outside. Through these protrusions, the seed flows into the cloaca of the female. Turtles, crocodiles have a penis, which is a thickening of the wall of the cloaca, which is supported by an erect cavernous tissue. Birds have a similar structure of the external genitalia. The penis is more perfectly represented in mammals. In some of them, the copulatory organ is located inside the cloaca and is able to exit and be drawn into the cloaca by special muscles. In viviparous mammals, the cloaca disappears, and the urogenital sinus and canal of the penis merge into a common urethra, through which urine and semen flow. The elasticity of the penis is maintained by erect cavernous and spongy tissue, and in many animals, additional bone tissue develops in the cavernous bodies of the penis and clitoris.
