Signs of gray matter heterotopia treatment. Subcortical heterotopia: lissencephaly
Keywords: epilepsy, focal cortical dysplasia, gray matter heterotopia, corticography
Target: evaluation of the results of surgical treatment of epilepsy in patients with impaired migration of neurons in the cerebral cortex.
Materials and methods: operated on 4 patients aged 20 to 37 years (2 men and 2 women) with epilepsy caused by various developmental disorders of the cerebral cortex.
results: all patients in the clinical picture had partial seizures with secondary generalization for 6 to 22 years before hospitalization. MRI of the brain revealed focal cortical dysplasia in three patients and diffuse periventricular heterotopia of the gray matter of the brain in one patient. Three patients with FCD underwent implantation of corticographic electrodes to determine the area of the cortex responsible for the development of seizures. Patients with FCD underwent topectomy of lesions with intraoperative corticography, a patient with periventricular heterotopia underwent lobectomy of the right frontal lobe. Infectious and neurological complications after the interventions were not observed. Morphological examination of preparations revealed Taylor type FCD in 2 patients, non-Taylor type FCD in one patient, and diffuse periventricular gray matter heterotopia in one patient. After 12 months in the postoperative period, in three patients with FCD, the result of surgical treatment was assessed as class IA according to the Engel scale (complete relief from seizures), in a patient with gray matter heterotopia - II according to the Engel scale (reduction in the frequency of seizures by 50%)
conclusions. In patients with drug-resistant epilepsy, it is necessary to take into account the possible etiopathogenetic role of disturbances in the migration of cortical neurons. Surgical treatment may be an option to achieve stable clinical remission and social adaptation of patients.
Schizencephaly is an anomaly in the structure of the cortex. It occurs due to a violation of the development of the brain at 2-5 weeks of pregnancy. The disease is associated with impaired migration of neurons to the cerebral cortex during the formation of brain neural networks.
Content:
What is schizencephaly?
Due to insufficient vascular nutrition or its absence, part of the brain tissue is not formed. Schizencephaly is not a process of tissue destruction, but a consequence of its underdevelopment (a linear defect in brain tissue characterized by the absence of gray matter cells).
The median age of symptom onset is 4 years (range 3–4 weeks to 12 years).
Schizencephaly is of two types.
Closed cleft - 1 type. It is characterized by a unilateral or bilateral linear section of the cerebral cortex with an imperfect structure. The walls of the clefts close, the ventricles communicate with the subarachnoid space. The cleft cavity is a small groove covered with ependymal epithelium and arachnoid meninges. It is not filled with cerebrospinal fluid, therefore it is impossible to diagnose pathology in the prenatal period of development on neurosonography.
Open (open) cleft - type 2. It can be seen on one or both sides. The walls of the defect are separated from each other by a lumen filled with CSF. Its length: from the walls of the ventricles to the subarachnoid space. On ultrasound, open schizencephaly is detected by an increase in the ventricles.
Symptoms
Closed schizencephaly accounts for more than 50% of all diagnosed cases. In 30% of cases, the disease is combined with progressive hydrocephalus, which is eliminated by ventricular shunting.The number and severity of symptoms depends on the type of schizencephaly: unilateral or bilateral, on the localization of the cortical defect.
Unilateral clefts cause paresis, partial or complete paralysis on one side of the body. Most children, when they grow up, have average mental abilities, the level of physical abilities is close to normal.
Signs of unilateral closed schizencephaly in most patients are limited to such developmental disorders: lack of initiative, lagging behind children of equal age mentally and physically (obviously during joint games), moderate speech perception disorders. Disturbances in coordination of movements are observed on the side of the body opposite the affected area.
bilateral clefts have more severe symptoms: delays in physical and mental development, difficulties in learning the language and teaching basic subjects at school. Due to imperfect connections between the brain and spinal cord, limitation of motor functions is possible. Bilateral incoordination is possible with bilateral (bilateral) schizencephaly, even with a small size of the clefts.
Other signs of schizenzfalia:
- low muscle tone;
- hydrocephalus (accumulation of fluid in the ventricles of the brain);
- microcephaly (head smaller than normal), sometimes macrocephaly (due to hydrocephalus);
- frequent seizures.
The head circumference of a newborn under the age of one with hydrocephalus can increase to 50-75 cm instead of the normal 40 cm at 3 months and 47 cm per year.
All children with schizencephaly are diagnosed with focal epilepsy.(a clearly defined zone of epiactivity).
Seizure types:
- Complex focal seizures - blurred consciousness, turning of the head, motionless fixation of the gaze, myoclonus (convulsive muscle twitches) of the lower extremities. Usually seen on only one side of the body.
- Complex seizures with secondary generalization (preceded by an aura or focal seizure).
- Simple seizures.
Less common are myoclonic (rhythmic twitches of muscle groups that provoke involuntary movements) and tonic (unexpected muscle relaxation) seizures. They can recur 4-8 times a month or less often, sometimes occur only a few times in a lifetime.
Frequency and severity of epileptic seizures does not depend on the type of schizencephaly, but on the presence of segments of cortical dysplasia (an abnormal structure of the cerebral cortex).
In 100% of cases, schizencephaly is characterized by a violation of higher cortical functions: vision, hearing, sensitivity (smell, touch, taste) of varying severity. Movement disorders are more pronounced with frontal localization of clefts.
Schizencephaly is rarely an independent pathology. Usually detected in combination with a group of anomalies, also formed as a result of violations of the processes of ontogenesis (development of the body) during pregnancy:
- dysgenesis(underdevelopment) or absence of the corpus callosum;
- ventriculomegaly(enlargement of the ventricles with a violation of the outflow of cerebrospinal fluid);
- cerebellar hypoplasia(responsible for motor functions and coordination);
- polymicrogyria(a lot of extra convolutions, incorrect arrangement of the layers of the cerebral cortex);
- gray matter heterotopia(abnormal accumulation and incorrect localization);
- dilatation(displacement) or wall defects, underdevelopment horns of the ventricles of the brain.
The clinical picture of schizencephaly is complemented by the consequences of a brain defect:
- hydrocephalic head shape (abnormally high forehead, enlarged upper part of the skull, superciliary ridges strongly outlined and shifted forward, strongly pronounced venous pattern on the forehead);
- violations of the innervation of the muscles that ensure the movement of the eyeballs, the internal muscles of the eye and eyelids;
- abnormal facial expressions or lack thereof due to improper innervation of the muscles of the face;
- bulbar palsy (disturbances of speech, swallowing, inability to control (move) the muscles of the face);
- increased muscle tone;
- spastic tetraparesis (paresis of all limbs, asymmetry and impaired muscle tone);
- absence or violation of unconditioned reflexes;
Sometimes the neurological signs of schizencephaly are less severe than doctors initially suspect from an MRI.
What causes schizencephaly?
The exact cause of schizencephaly is unspecified. Most researchers put forward theories related to genetic and vascular disorders.
Mutations in the homeobox genes responsible for the growth and migration of neuroblasts (progenitors of neurons) are seen in many but not all children with schizencephaly. The genetic theory of occurrence is supported by cases of schizencephaly in siblings.
The development of the disease may be affected infections (for example, cytomegalovirus) and medicines .
What processes provoke the appearance of space in the gray matter?
Others express a different opinion: clefts in the gray matter are formed as a result of vascular occlusion . Blockage or absence of the internal carotid or middle cerebral arteries leads to ischemic stroke and subsequently to brain necrosis.
Diagnostics
Examination and symptomatic treatment are carried out in the psycho-neurological department.Doctors use the following instrumental diagnostic methods:
- Magnetic resonance imaging.
- X-ray computed tomography.
- Electroencephalography is supplemented by tests with opening and closing the eyes, photostimulation and hyperventilation (the child is asked to inhale and exhale quickly and deeply).
In all children with schizencephaly, the EEG shows a slowdown in background activity, as well as one of two changes:
- local epileptic activity in the frontotemporal regions;
- ubiquitous epileptic activity without a specific focus.
Due to the presence of hydrocephalus, open schizencephaly is similar to porencephaly , however, in the second case, the cleft is not covered with epithelial, but with connective or glial (auxiliary) tissue. The disease may be confused with holoprosencephaly (complete or partial absence of division of the forebrain into hemispheres).
CT is rarely used in the diagnosis of schizencephaly, as MRI provides a more complete picture of the pathology.

With the help of magnetic resonance imaging, concomitant disorders of brain development are detected:
- gray matter heterotopia (nodules in the gray matter under the lining of the ventricles);
- optic nerve hypoplasia (insufficient number of axons, structural units of neurons);
- agenesis of the septum pellucidum in frontal localization of schizencephaly;
- septo-optic dysplasia (developmental disorders of the pituitary gland, septum pellucidum, optic nerve).
Treatment
Symptomatic treatment of schizencephaly is provided.
Tetraparesis, hemiparesis, convulsions, muscle spasticity, psychomotor retardation, are treated with electrical stimulation or micropolarization of the brain, psychotherapy, antiepileptic drugs, botulinum therapy (blocking the transmission of unwanted signals from nerves to muscles), orthopedic treatment is used.
Patients with mild schizencephaly do not experience relapses after starting treatment with antiepileptic drugs.
What doctors other than a neurologist and a neurosurgeon will help a child?
Doctors in at least 3 specialties can help improve quality of life:
- Physiotherapist will prescribe therapy to improve the prognosis of the development of motor skills, namely: the ability to sit and stand (in severe cases). Children with mild symptoms may benefit from exercises to strengthen the muscles in their arms and legs.
- Services occupational therapist will be needed if the child cannot perform actions that require well-developed fine motor skills: eat, dress on their own. Occupational therapy will make available a full life and the performance of functions at home, in kindergarten, school.
- Speech therapist improve speaking and swallowing skills.
What is the prognosis?
Schizencephaly has a predominantly favorable prognosis for life. In the case of timely provision of resuscitation and / or rehabilitation measures and subsequent treatment, remission occurs. Problems with motor activity will persist for life, there is a risk of mental retardation, but most patients can live fully in society.In addition to epilepsy, hydrocephalus is the main problem in patients with schizencephaly. With a constant increase in fluid on the one hand, there is a displacement of the ventricles and compression of the surrounding tissues, including the medulla oblongata (regulates the activity of the heart and respiratory function). Moderate hydrocephalus is treated pharmacologically, but not always doctors can offer options other than bypass surgery.
The story of a small patient: a boy, 2 years old.
Mother - 25 years old, father - 29 years old, first pregnancy, satisfactory health, absence of harmful environmental factors in the area of residence and at work.
Hydrocephalus was first suggested by ultrasound at 34 weeks. From the district clinic, the patient was referred to the regional perinatal center.
The size of the fetus on fetometry corresponded to the gestational age. When examining the brain in the right hemisphere, a cavity with liquid contents was noted. The vascular glomeruli in it made it possible to make sure that the cause of its formation was not a cyst. Apart from the open circle of Willis, no other changes were found.
The clinical diagnosis was made: schizencephaly type 2 (with an open cleft). After 5 weeks, a male child was born. Weight: 3450 g, 7 points on the Apgar scale. Immediately after birth, an NSG was performed, the diagnosis was confirmed. The mother and child were discharged from the hospital on the 4th day.
It's been 2 years. The child is far behind peers in psychomotor development (statics, motor skills, sensory reactions, speech, social interaction), motor abilities are limited. There is a convulsive syndrome and a decrease in spinal reflexes.
The presence of craniofacial anomalies, which can be seen visually, has a negative prognostic value: microcephaly, hydrocephalic head shape. Similar deviations can develop in a child with open schizencephaly.
A favorable prognosis for life will be given to the child with closed schizencephaly. Open clefts in the gray matter, on the contrary, lead to a delay in mental or psycho-speech development (ZPR or ZPRR), movement disorders.
History of an adult patient: 20 years.
Handling complaints of torticollis (noise and ringing in the ears), epileptic seizures with speech automatisms (uncontrolled pronunciation of words), tonic-clonic convulsions. Epilepsy attacks lead to loss of consciousness.
From the moment of birth until the admission to the hospital after the last seizure, which happened in class at the university, the diagnosis of schizencephaly was not assumed.
Brief anamnesis. At birth, no abnormalities were noted, developmental delay began at 9 months, the right side abruptly ceased to obey. After contacting a pediatric neurologist, they did an MRI and CT scan, diagnosed with cerebral palsy (later it turned out that the diagnosis was incorrect). A course of vasoactive and neurometabolic drugs was prescribed, although there were no corresponding indications.
The first seizure of epilepsy occurred at the age of 8. Subsequently, seizures were observed with auditory aura and severe convulsions, but without loss of consciousness. Many drugs were prescribed, including antiepileptic drugs, but the disease progressed.
Recently, attacks began a few days before or at the beginning of menstruation. For the treatment of epilepsy, a course of Depakine was prescribed in combination with Lamictal. The number of seizures decreased, but if they started, there were several seizures per day.
The results of diagnostics when contacting the regional clinical hospital. The EEG showed moderate changes in bioelectrical activity, an irregular alpha rhythm, epiactivity in the temporal region of the left hemisphere. The MRI picture is characteristic of schizencephaly.
Appearance defects: divergent strabismus, asymmetry of the nasolabial zone, gothic (high and narrow, arched) palate, the shape of the dental arches is broken, ichthyosis (dry, scaly skin) in the shins, the right arm and leg are shortened by 2 and 2.5 cm.
Neurological problems: astigmatism (partial blurring of the contours of images, blurred vision), on the right side of the body there is an increase in tendon reflexes (cramps in the muscles during stretching), paraparesis (decrease in muscle activity), decreased sensitivity. Unsteady in the Romberg position (standing straight with outstretched arms). Polyneuropathy (decreased sensitivity in the arms below the elbow, hypersensitivity in the legs below the knee).
A pessimistic prognosis is given to children with drug-resistant epilepsy (that is, with seizures that cannot be controlled by drugs). The presence of comorbidities worsens the quality of life and reduces the available opportunities.
A lethal outcome is possible with acute infections (including those that have become chronic), metabolic disorders, severe toxicosis, and multiple organ failure.
Subependymal heterotopia(periventricular heterotopia) is the most common form of gray matter (SG) heterotopia, characterized by SG nodules located directly below the ependyma of the lateral ventricles. According to morphology can be divided into:
- unilateral focal
- bilateral focal
- bilateral diffuse: a wavy strip of SW surrounding the ventricles.
Epidemiology
Most cases are sporadic, some are X-linked recessive (Xq28). Women have relatively mild cognitive impairment, subsequently developing epilepsy. In the case of boys, spontaneous abortion occurs, usually due to malformations of the cardiovascular system. The survivors are severely disabled.
Clinical picture
Most often, subependymal heterotopia is associated with epilepsy and developmental delay.
Pathology
Like other types of heterotopias, this type is the result of a violation of neuronal migration. In some cases, the cause of the development of subependymal heterotopia is a violation of cell proliferation.
Gray matter nodules are composed of clusters of neurons and glial cells. It is interesting to note that they are most often found on the right side, presumably due to later migration of neuroblasts from the right side.
X-linked cases show mutations in the gene for filamin-1, a protein that cross-links intracellular actin. In addition, filamin-1 also plays an important role in vascular development.
Diagnostics
MRI is the modality of choice, although periventricular heterotopia is seen on CT and ultrasonography (if the size is very large).
ultrasound
Subependymal SW nodules are usually hyperechoic compared to normal white matter, and they may also protrude into the ventricular lumen (ventricular undulations).
CT
On CT, subependymal heterotopia appears as a non-calcified area of tissue that does not accumulate contrast agent, similar in density to normal gray matter, around the lateral ventricles.
MRI
Antenatal MRI
In late pregnancy, the diagnosis of subependymal heterotopia is relatively clear. Before 26 weeks of gestation, the presence of a normal teleencephalic periventricular germinal matrix makes it difficult to detect, as does fetal movement.
Postnatal MRI
Small nodules of gray matter are observed in the ependymal layer and distort the contour of the ventricles. Most often, localization is in the region of the triangle and occipital horns. Other areas of the brain appear normal.
Gray matter nodules are visualized on all sequences, including post-contrast ones, where, like normal gray matter, they do not accumulate contrast agent.
Differential Diagnosis
- norm
- caudate nuclei
- thalamus
- subependymal giant cell astrocytoma
- has a pronounced accumulation of contrast
- localized near the foramen of Monroe
- subependymal nodes in tuberous sclerosis
- usually calcified (except in early childhood)
- higher T2 signal than gray matter signal
- subependial hemorrhage on ultrasound and antenatal MRI
- although the picture may be similar, the control study in the case of hemorrhage determines the evolution of changes
This is the result of disturbances in the formation of individual cerebral structures or the brain as a whole that occur in the prenatal period. They often have nonspecific clinical symptoms: predominantly epileptic syndrome, mental and mental retardation. The severity of the clinic directly correlates with the degree of brain damage. They are diagnosed antenatally during obstetric ultrasound, after birth - using EEG, neurosonography and MRI of the brain. Symptomatic treatment: antiepileptic, dehydration, metabolic, psychocorrective.
ICD-10
Q00 Q01 Q02 Q04

General information
Anomalies in the development of the brain - defects, consisting in abnormal changes in the anatomical structure of cerebral structures. The severity of neurological symptoms accompanying cerebral anomalies varies considerably. In severe cases, malformations are the cause of antenatal fetal death, they account for up to 75% of intrauterine deaths. In addition, severe cerebral anomalies cause about 40% of newborn deaths. The timing of the manifestation of clinical symptoms may be different. In most cases, cerebral anomalies appear in the first months after the birth of a child. But, since the formation of the brain lasts until the age of 8, a number of defects make their debut clinically after the 1st year of life. In more than half of the cases, cerebral malformations are combined with malformations of somatic organs. Prenatal detection of cerebral anomalies is an urgent task of practical gynecology and obstetrics, and their postnatal diagnosis and treatment are priority issues of modern neurology, neonatology, pediatrics and neurosurgery.
The reasons
The most significant cause of intrauterine development failures is the impact on the body of a pregnant woman and on the fetus, various harmful factors that have a teratogenic effect. The occurrence of an anomaly as a result of monogenic inheritance occurs only in 1% of cases. The most influential cause of brain defects is considered to be an exogenous factor. Many active chemical compounds, radioactive contamination, and certain biological factors have a teratogenic effect. Of no small importance here is the problem of pollution of the human environment, which causes the intake of toxic chemicals into the body of a pregnant woman.
Various embryotoxic effects may be associated with the lifestyle of the pregnant woman herself: for example, smoking, alcoholism, drug addiction. Dysmetabolic disorders in a pregnant woman, such as diabetes mellitus, hyperthyroidism, etc., can also cause fetal cerebral anomalies. Many medications that a woman can take in the early stages of pregnancy, unaware of the processes taking place in her body, also have a teratogenic effect. A powerful teratogenic effect is exerted by infections carried by a pregnant woman or intrauterine infections of the fetus. The most dangerous are cytomegaly, listeriosis, rubella, toxoplasmosis.
Pathogenesis
The construction of the fetal nervous system begins literally from the first week of pregnancy. Already by the 23rd day of gestation, the formation of the neural tube ends, the incomplete fusion of the anterior end of which entails serious cerebral anomalies. By about the 28th day of pregnancy, the anterior cerebral vesicle is formed, which subsequently divides into 2 lateral ones, which form the basis of the cerebral hemispheres. Further, the cerebral cortex, its convolutions, the corpus callosum, basal structures, etc. are formed.
Differentiation of neuroblasts (germ nerve cells) leads to the formation of neurons that form the gray matter and glial cells that make up the white matter. The gray matter is responsible for the higher processes of nervous activity. In the white matter, there are various pathways that connect the cerebral structures into a single functioning mechanism. A newborn born at term has the same number of neurons as an adult. But the development of his brain continues, especially intensively in the first 3 months. life. There is an increase in glial cells, branching of neuronal processes and their myelination.
Failures can occur at various stages of brain formation. If they occur in the first 6 months. pregnancy, they can lead to a decrease in the number of formed neurons, various disorders in differentiation, and hypoplasia of various parts of the brain. At a later date, damage and death of a normally formed cerebral substance may occur.
Types of brain anomalies
Anencephaly- Absence of the brain and acrania (lack of skull bones). The place of the brain is occupied by connective tissue growths and cystic cavities. May be covered in leather or naked. Pathology is incompatible with life.
encephalocele- prolapse of cerebral tissues and membranes through a defect in the bones of the skull, due to its non-closure. As a rule, it is formed along the midline, but it can also be asymmetric. A small encephalocele may mimic a cephalohematoma. In such cases, x-ray of the skull helps determine the diagnosis. The prognosis depends on the size and contents of the encephalocele. With a small protrusion and the presence of ectopic nervous tissue in its cavity, surgical removal of the encephalocele is effective.
Microcephaly- a decrease in the volume and mass of the brain, due to a delay in its development. It occurs with a frequency of 1 case per 5 thousand newborns. Accompanied by a reduced head circumference and a disproportionate ratio of the facial / brain skull with a predominance of the first. Microcephaly accounts for about 11% of all cases of mental retardation. With severe microcephaly, idiocy is possible. Often there is not only ZPR, but also a lag in physical development.
Macrocephaly- an increase in the volume of the brain and its mass. Much less common than microcephaly. Macrocephaly is usually combined with impaired brain architectonics, focal white matter heterotopia. The main clinical manifestation is mental retardation. There may be a convulsive syndrome. There is partial macrocephaly with an increase in only one of the hemispheres. As a rule, it is accompanied by asymmetry of the cerebral part of the skull.
Cystic cerebral dysplasia- characterized by multiple cystic cavities of the brain, usually connected to the ventricular system. Cysts can vary in size. Sometimes localized only in one hemisphere. Multiple brain cysts present with epilepsy that is resistant to anticonvulsant therapy. Single cysts, depending on the size, may have a subclinical course or be accompanied by intracranial hypertension; their gradual resorption is often noted.
Holoprosencephaly- lack of separation of the hemispheres, as a result of which they are represented by a single hemisphere. The lateral ventricles are formed into a single cavity. Accompanied by gross dysplasia of the facial skull and somatic defects. Stillbirth or death is noted on the first day.
focal cortical dysplasia(FKD) - the presence in the cerebral cortex of pathological areas with giant neurons and abnormal astrocytes. Favorite location - temporal and frontal areas of the brain. A distinctive feature of epileptic seizures in PKD is the presence of short-term complex paroxysms with rapid generalization, accompanied in their initial phase by demonstrative motor phenomena in the form of gestures, trampling in one place, etc.
Heterotopia- accumulations of neurons, at the stage of neuronal migration, delayed on their way to the cortex. Heterotopions can be single and multiple, have a nodal and ribbon shape. Their main difference from tuberous sclerosis is the lack of ability to accumulate contrast. These anomalies in the development of the brain are manifested by episyndrome and oligophrenia, the severity of which directly correlates with the number and size of heterotopions. With solitary heterotopia, epileptic seizures usually debut after 10 years of age.
Diagnostics
Severe brain anomalies can often be diagnosed by visual examination. In other cases, ZPR, muscle hypotension in the neonatal period, the occurrence of convulsive syndrome in children of the first year of life allows suspecting a cerebral anomaly. It is possible to exclude the traumatic or hypoxic nature of brain damage if there is no history of data on birth trauma of the newborn, fetal hypoxia or asphyxia of the newborn. Prenatal diagnosis of fetal malformations is carried out by screening ultrasound during pregnancy. Ultrasound in the first trimester of pregnancy can prevent the birth of a child with a severe cerebral anomaly.
One of the methods for detecting brain defects in infants is neurosonography through the fontanel. Much more accurate data in children of any age and in adults is obtained using MRI of the brain. MRI allows you to determine the nature and localization of the anomaly, the size of cysts, heterotopias and other abnormal areas, to conduct differential diagnosis with hypoxic, traumatic, tumor, infectious brain lesions. Diagnosis of convulsive syndrome and the selection of anticonvulsant therapy is carried out using EEG, as well as prolonged EEG video monitoring. In the presence of family cases of cerebral anomalies, it may be useful to consult a geneticist with genealogical research and DNA analysis. In order to identify combined anomalies, an examination of somatic organs is carried out: ultrasound of the heart, ultrasound of the abdominal cavity, radiography of the chest organs, ultrasound of the kidneys, etc.
Treatment of brain anomalies
Therapy of malformations of the brain is predominantly symptomatic, carried out by a pediatric neurologist, neonatologist, pediatrician, epileptologist. In the presence of a convulsive syndrome, anticonvulsant therapy is performed (carbamazepine, levetiracetam, valproates, nitrazepam, lamotrigine, etc.). Since epilepsy in children accompanying brain developmental anomalies is usually resistant to anticonvulsant monotherapy, a combination of 2 drugs is prescribed (for example, levetiracetam with lamotrigine). With hydrocephalus, dehydration therapy is carried out, according to indications, bypass surgery is resorted to. In order to improve the metabolism of normally functioning brain tissues, which to some extent compensate for the existing congenital defect, it is possible to conduct a course of neurometabolic treatment with the appointment of glycine, vitamins gr. B etc. Nootropic drugs are used in the treatment only in the absence of episyndrome.
With moderate and relatively mild cerebral anomalies, it is recommended that a comprehensive psychological support for the child, teaching older children in specialized schools. These methods help to instill self-service skills, reduce the severity of oligophrenia and, if possible, socially adapt children with cerebral malformations.
Forecast and prevention
The prognosis is largely determined by the severity of the cerebral anomaly. An unfavorable symptom is the earlier onset of epilepsy and its resistance to ongoing therapy. The presence of concomitant congenital somatic pathology complicates the prognosis. An effective preventive measure is the exclusion of embryotoxic and teratogenic effects on a woman during pregnancy. When planning a pregnancy, future parents should get rid of bad habits, undergo genetic counseling, and be examined for chronic infections.

The main morphological parts of the brain
- the forebrain (final) brain consists of two cerebral hemispheres.
- The diencephalon consists of the thalamus, epithalamus, hypothalamus, pituitary gland, which is not included in the diencephalon, but is isolated into a separate gland.
- the midbrain consists of the legs of the brain and the roof of the quadrigemina. The upper hills of the roof of the quadrigemina are the subcortical visual center, and the lower hills are the subcortical center of hearing.
- the hindbrain consists of the pons and cerebellum.
- medulla. The junction of the medulla oblongata with the spinal cord is the foramen magnum.
The midbrain, hindbrain and medulla oblongata are combined into a brainstem.

The internal structure of the cerebral hemispheres.
- Gray matter
- white matter
The gray matter consists of the cortex, which completely covers the cerebral hemispheres. The white matter is located under the gray matter of the brain. However, areas with gray matter are also present in the white matter - clusters of nerve cells. They are called nuclei (nuclei). Normally, there is a clear boundary between white and gray matter. Differentiation of white and gray matter is possible on CT, but better differentiated on MRI.

Cortical dysplasia
In cortical dysplasia, the boundaries between white and gray matter are blurred. In such a case, the sequence T1 recovery inversion should be additionally used. On these images, the borders will be visible, except for areas of cortical dysplasia.

heart attack
With cytotoxic edema, which develops in the first minutes of cerebral infarction, differentiation between white and gray matter is also lost, which is an early CT sign of cerebral infarction.







Large hemispheres of the brain
The hemispheres of the brain are separated by a large falciform process. There are 4 lobes in each hemisphere:
- frontal lobe.
- parietal lobe
- occipital lobe
The frontal lobe is separated from the parietal by means of a central or raland groove, which is perfectly visualized both on axial and sagittal sections.
The frontal lobe is separated from the temporal lobe by a lateral groove, which is excellently visualized both on sagittal and axial, and on frontal sections.
The parietal lobe is separated from the occipital lobe by the parietal-occipital sulcus of the same name. This line still separates the carotid and basilar pools.
Some authors allocate an island in a separate groove, which is a large area of the cortex covering the island from above and laterally, forms an operculum (Latin pars opercularis) and is formed from part of the adjacent frontal, temporal and parietal lobes.
Share boundaries


Share boundaries
Borders of the frontal and parietal lobes.
Omega -?
central sulcus
mustache symptom- Postcentral gyrus.
cingulate gyrus – postcentral gyrus.
To correctly determine the border of the frontal and parietal lobes, we first find the central sulcus. The symbol is inscribed in this groove Omega -? on axial sections.
The symptom of a mustache located perpendicular to the midline and an image that corresponds to the postcentral sulcus also help. Anterior to the postcentral gyrus, respectively, the central sulcus is located.
Belt furrow.
On sagittal sections, you need to find the corpus callosum above it there is a cingulate sulcus, which continues posteriorly and upwards into the postcentral sulcus, from which the central or Roland sulcus is located anteriorly.

frontal lobe
The frontal lobe is large and one of the main gyrus is the precentral gyrus, which is the cortical center of movement. In the frontal lobe, the superior, middle, and inferior gyrus are also noted. The listed convolutions go from top to bottom and parallel to each other.
On the lower surface of the frontal lobe are straight and orbital gyri, between which are the olfactory tracts and bulbs. These areas are damaged by trauma.

Traumatic injury to the frontal lobe
In this patient, we note symmetrical damage to the basal sections of both frontal lobes, which correspond to post-traumatic changes.

Broca's area
Also an important area is Broca's area, which is located in the distal parts of the inferior frontal gyrus. Its localization is important when planning neurosurgical interventions. This zone is easy to find, remembering the McDonald's icon.

Infarction with involvement in the pathological process Broca's area
This patient has an acute infarction due to occlusion of the anterior M2 branch of the left MCA. Damage to the frontal lobe with involvement in the pathological process of Broca's area.

parietal lobe
Behind the central sulcus is the postcentral gyrus, which serves as a cortical analyzer of general and proprioceptive sensitivity.
Behind are the upper and lower parietal lobules.
In the upper parietal lobule is the core of the skin analyzer responsible for stereognosia - the ability to recognize objects by touch.
In the lower parietal lobule there is a motor analyzer responsible for apraxia - purposeful and voluntary movements.
stereognosia- the ability to recognize objects by touch.
Apraxia- violation of arbitrary actions.

Atrophy of the precuneus
Atrophy of the precuneus is an early symptom of Alzheimer's disease even before atrophy of the cortex of the temporal lobes and the hippocampus.
The precuneus is a section of the parietal lobe on the inner surface of both cerebral hemispheres, located above and in front of the corpus callosum.

temporal lobe
In the temporal lobe secrete
superior temporal gyrus
Middle temporal gyrus
Inferior temporal gyrus. These three convolutions are parallel to each other and are located in a horizontal plane.
Geschl's convolutions are located on the surface of the superior temporal gyrus. They are the cortical center of hearing.
The parahippocampal gyrus is located on the lower surface of the temporal lobes in the medial regions. The hook together with the hippocampus are responsible for the sense of smell. When the hippocampus is damaged, memory is impaired in the first place.
Wernicke's area. Wernicke's area is located in the distal parts of the superior temporal gyrus. It is a sensory speech zone.

Occipital lobe
In the occipital lobes, irregular furrows and convolutions are determined, but the most constant is the spur groove located on the medial surface of the occipital lobe. Around the spur groove are 17, 18 and 19 Brodmann fields, which are the cortical center of vision.

Occlusion of the PCA
This patient has clinically observed visual impairment due to damage to the occipital lobe, the cause of which was a heart attack (occlusion of the PCA).
subcortical gray matter







subcortical gray matter
The subcortical gray matter includes:
- thalamus
- basal nuclei
- caudate nucleus
- lenticular nucleus, in which the shell and pale ball are isolated.
- shell
The internal capsule consists of the anterior thigh, knee and posterior thigh.
How to find the hind thigh?
Between the thalamus and the lenticular nucleus we find a hyperintense focus, which is a pyramidal tract. From this hyperintense focus, we draw a line to the knee, which will be the projection of the posterior femur of the internal capsule.
NB - Do not confuse the back knee with the pale ball.
When classifying intracerebral hemorrhages in the subcortical gray matter, depending on the location in relation to the internal capsule, hemorrhages are divided into:
- lateral
- medial
- mixed
WHITE MATTER
Commissural fibers that connect the hemispheres.
Corpus callosum (largest commissure)
Anterior commissure
Posterior commissure (commissure of the fornix)

Anterior commissure
The anterior commissure is located under the beak of the corpus callosum behind the end plate and connects some parts of the olfactory brain: the hippocampal gyrus, the left and right hooks of the temporal lobes.
Posterior commissure
The posterior commissure belongs to the epithalamus, is located at the root of the epiphysis and connects the corresponding parts of the midbrain and diencephalon.
Practical value:
The bicommissural line in the sagittal plane is used to assess the corpus callosum. The bicommissural line is drawn through the upper edge of the anterior commissure and the lower edge of the posterior commissure.

corpus callosum
The corpus callosum consists of:
Trunk or body (anterior and posterior)
Each section connects the homolateral section of the brain.
Formation of the corpus callosum.
The corpus callosum develops in a special order:
From the knee, then the body, the roller and at the end the beak develops.
Myelination of the corpus callosum proceeds from the posterior to the anterior regions.
This knowledge helps to narrow the differential diagnosis in pathologies of the corpus callosum.

Dysgenesis and atrophy of the corpus callosum
With dysgenesis of the corpus callosum, the knee and anterior parts of the corpus callosum are well formed, but the ridge and beak are absent. This pathology is congenital. The pathology is shown on the left.
With atrophy of the corpus callosum, the posterior sections of the corpus callosum (posterior section of the body and roller) are well formed, but the beak, knee and anterior section of the body are reduced in size. These changes are acquired.
Many diseases affect the corpus callosum, so the presence of lesions is not pathognomonic for a particular disease.

Marchiafava-Bignami disease
Marchiafava-Bignami disease (central degeneration of the corpus callosum, Marchiafava syndrome, extrapontine myelinolysis).
It occurs in people who abuse alcohol. In these individuals, MRI reveals a lesion of the ridge and posterior parts of the trunk (body) of the corpus callosum.
In the chronic stages of Marchiafava-Bignami disease, the corpus callosum is visualized in the form of a sandwich, in which the upper and lower layers of the corpus callosum are preserved, but with necrosis of the middle layers.
white matter
White matter:
- periventricular
- deep sections (semioval centers)
- U-fibers
The periventricular white matter is located in close proximity to the lateral ventricles of the brain.
U-fibers connect the cortex of nearby gyri or subcortical white matter.
Deep sections of white matter located between the periventricular and subcortical white matter.
Lesions in white matter:
White matter lesions are classified according to location:
- periventricular
- juxtacortical
- subcortical
- lesions in deep white matter

Periventricular lesions
periventricular (single or multiple, small or large, merging with each other)

Juxtacortical lesions
juxta - approx. These foci are localized in u-fibers and are directly adjacent to the gray matter, that is, there is no layer of white matter between the lesion and the gray matter.
In shape, these foci are different, how to repeat the shape of u-fibers, they can also be rounded and irregular in shape. This localization is pathognomonic for MS.

Subcortical lesions
Subcortical foci are foci that are localized near the cerebral cortex, but at the same time there is a layer of white matter between the focus and the cortex.

Foci in deep white matter.
These foci are found in various diseases of the brain.




VENTRICLES OF THE BRAIN
The lateral ventricles are composed of:
- anterior (frontal) horns
- posterior (occipital) horns
- lower (temporal) horns
The lateral ventricles are connected to the third ventricle by the paired foramen of Monro.
The third ventricle has an irregular shape due to the presence of pockets. The opening of the third ventricle corresponds to the interthalamic commissure.
The third ventricle is connected to the fourth ventricle by a sylvian aqueduct. From the fourth ventricle, the CSF enters the basal cisterns through the paired foramina of Luschka and the unpaired aperture of Mogendi.
When evaluating the ventricles, it is worth paying attention to the ventricular horns, as in degenerative diseases such as Alzheimer's disease, atrophy of the hippocampus is accompanied by expansion of the temporal horns. In FLAIR mode, the signal from the posterior (occipital) horns is increased, which is normal as well as the asymmetry of the horns.
THIRD VENTRICLE.
The third ventricle is located in the midline between the visual tubercles. It connects to the lateral ventricles through the openings of Monroe, and to the fourth ventricle through the aqueduct of the brain.
Pockets of the third ventricle:
- suprachiasmatic
- Infundibullary
- Suprapineal
- Pineal
Normally, these pockets have sharp corners, but with increasing pressure, the pockets open.
The fourth ventricle of the brain.
The fourth ventricle is the cavity of the hindbrain and, with the help of the paired holes of Luschka and the unpaired hole of Magendie, is connected to the basal cisterns.

Vascular plexuses
CSF-producing choroid plexuses are located in all ventricles of the brain, so choroid plexus calcification, which is more often visualized in the posterior horns of the lateral ventricles, can be seen in both the third and fourth ventricles.

tuberous sclerosis.
Calcification of the choroid plexuses, which is the norm, should not be confused with pathological conditions. For example, with calcifications of the lateral ventricles - periventricular tubers in tuberous sclerosis.

Heterotopic gray matter
It is important to remember that the only gray matter bordering the lateral ventricles is the caudate nuclei, which have clear, even contours. Additional gray matter structures that deform the contour of the lateral ventricles are pathological changes characteristic of gray matter heterotopia.

Variants of the structure of the ventricles
- the cavity of the transparent septum, which is noted in most newborns (closes over time) and looks like a triangular shape between the bodies of the anterior lateral ventricle. This cavity never crosses the foramen of Monroe.
- the cavity of the intermediate sail. One of the walls of the cavity, which forms the roof of the third ventricle.
- Verge's cavity is an extended cavity between the bodies of the lateral ventricles.

colloid cyst
Structural variants should be distinguished from a colloid cyst, which will differ from the intensity of the signal from the cerebrospinal fluid in almost all pulse sequences. After the introduction of a contrast agent, colloid cysts do not accumulate contrast, which corresponds to a benign process.

MRI norm - median sagittal section. CSF - tanks.
A - END PLATE TANK
B - CASTERN OF CHIASMA
C - Interpeduncular cistern
D - Bypass tank
E - Quadrigeminal cistern
F - Cisternocerebellar cistern
G - Cisternocerebellar cistern Prepontine pontocerebellaris
H - LATERAL CEREBELLOMEDULLAR CASTERNA
I - TANK MAGNA
Image courtesy of Dr. Coenraad J. Hattingh
CANS OF THE BRAIN
From the fourth ventricle of the brain, the cerebrospinal fluid enters the basal cisterns with the help of the paired holes of Luschka and the unpaired hole of Magendie.
The name of the tanks, based on the localization:
In the sagittal plane:
- Suprasellar cistern
- Bridge cistern in which the main artery passes.
- Four hill cistern
- Large or basal cistern of the brain
In the axial plane:
- Interpeduncular cistern
- The bypass cistern connects the interpeduncular and quadrigeminal cistern. Also, wings are distinguished from the bypass tank: right and left.


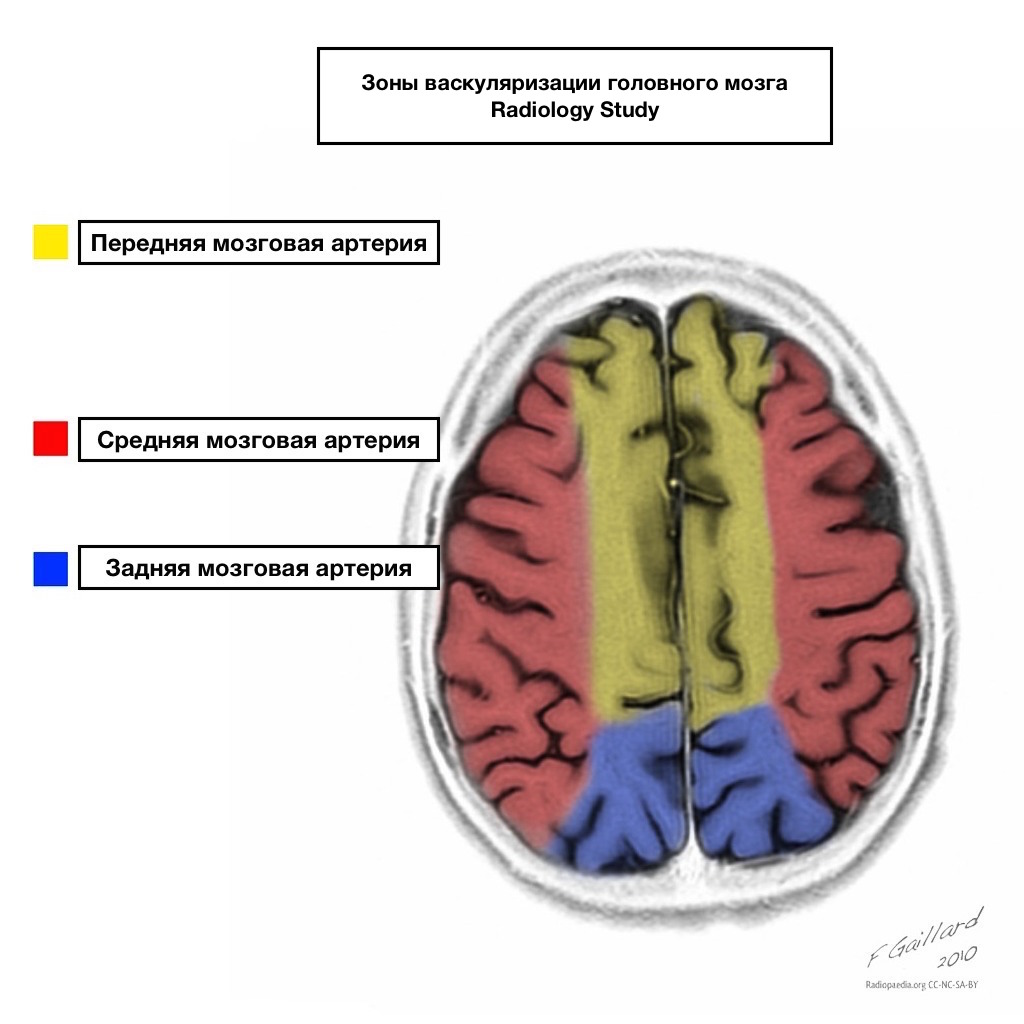







Pools of blood supply have clear boundaries.

Areas of adjacent blood supply
Zones of adjacent blood supply at the intersection of blood supply zones:
anterior cerebral artery
middle cerebral artery
Posterior cerebral artery.
Most often, infarctions in these areas are hemodynamic in nature, that is, they occur when blood pressure falls.

Shells of the brain
The brain is covered with three membranes.
- The soft shell is tightly attached to the brain, goes into all the cracks and furrows, and blood vessels are located in it. In certain places, it penetrates the ventricles of the brain and forms the choroid plexus.
- The arachnoid or arachnoid membrane lies over the furrows and spreads from one gyrus to another.
- The hard shell from the inside lines the cavities of the skull, adheres tightly to them and forms venous sinuses and processes that separate individual structures of the brain from each other.
Normally, the membranes of the brain are not visualized on MRI, but after the introduction of contrast, the dura mater is contrasted.

Changes in the soft meninges.
In leptomeningeal carcinomatosis, on T1 and T2 non-contrast images, there is an increase in the signal from the meninges, and after the introduction of contrast, it improves visualization.

Meningitis
Changes in the meninges are also often found in inflammatory changes, for example, in tuberculous leptomeningitis.

Dura change
A change in the dura mater occurs with intracranial hypotension. With this pathology, a thickened dura mater is visualized, intensively accumulating contrast. Additional criteria in the diagnosis is an increase in the size of the pituitary gland, prolapse of the cerebellar tonsils into the foramen magnum.

Changes in the dura mater also occur in pachymeningeal carcinomatosis, which is manifested by thickening of the dura mater with intense accumulation of contrast agent and vasogenic edema of the adjacent parts of the frontal lobe.
![]()
Shell spaces.
Shell spaces are the spaces between the shells of the brain.
- The subarachnoid space is the space between the pia mater and the arachnoid. Normally, it should have the intensity of cerebrospinal fluid.
- The subdural space is the space between the arachnoid and the dura.
- The epidural space is the space between the dura and the bones of the skull, which is not normally visualized as the dura is fused to the bones of the skull.

Change in the subarachnoid space
Change in the subarachnoid space
Narrowing. These changes occur during volumetric exposure (tumor, infarction).
Extension. These changes occur in the post-traumatic period, after a heart attack, or during atrophy.



Shell hemorrhages
With shell hemorrhages, we can perfectly identify the shells.
Types of shell hemorrhages:
epidural hemorrhage. Usually seen as a lens and do not extend beyond the sutures, but may cross the sinuses of the brain, which is different from subdural hemorrhages, which never cross the sinuses of the brain.
Subdural hemorrhage. The most common cause is rupture of superficial veins as a result of displacement of the brain during trauma. If in this case the subarachnoid membrane also ruptures, then in this case the cerebrospinal fluid enters the subdural space.
Subarachnoid hemorrhage. An increase in the signal from the cerebrospinal fluid in the FLAIR mode is detected. The most common cause of subarachnoid hemorrhage is an aneurysm rupture, as the arteries supplying the brain are localized in the subarachnoid space.

In pathological processes in the shells, the term lobes is not used, but instead the term region is used. For example, this patient has frontal meningioma.
