Blood supply to the hip joint. Collateral circulation in the hip joint
The hip joint is the largest articulation in the human musculoskeletal system, connecting the lower limbs to the body. Takes an active part in the movement and maintaining balance in the vertical position of the body. Despite its strength, the hip joint is one of the most vulnerable parts of the human skeleton, as it experiences daily stress when walking, running and exercising.
Human hip anatomy
The hip joint is a large spherical joint with several axes of rotation, formed by the articular surface of the femoral head and the acetabulum of the ilium of the pelvis. The structure of the hip joints in women and men has no fundamental differences.
In fact, the hip joint consists of a neck and a head covered with cartilaginous tissue, a femoral bone, an acetabulum and an acetabular lip deepening it, located inside the capsule. The articular capsule of the hip joint is a hollow formation that limits its internal cavity. The walls of the capsule consist of three layers:
- external - dense fibrous tissue;
- median - connective tissue fibers;
- internal - synovial membrane.
The synovial membrane lining the joint capsule from the inside produces a serous secretion that acts as a lubricant for the articular surfaces during movement, reducing their friction against each other.
Articular ligaments
The ligamentous apparatus of the hip joint provides rotation, supination, as well as mobility of the lower extremities in the longitudinal and transverse directions; It is formed by several structures: 
- The iliofemoral ligament is the largest and strongest of all that holds and provides mobility to the hip joint. It originates near the anterior lower spine of the pelvic bone, and then fan-shaped, attaching in bundles in the femur along the intertrochanteric line. It is included in the group of muscles and ligaments responsible for balance and keeping the torso in an upright position. Another function of the ligament is to inhibit hip extension.
- Ischio-femoral - one end is attached to the ischium; passing inside the trochanteric fossa, the other end is woven into the articular capsule. Inhibits adductor movements of the hip.
- Pubic-femoral - originates on the anterior surface of the pubic bone and is woven into the joint capsule. Responsible for the inhibition of hip movements performed in a direction transverse to the axis of the body.
- The circular ligament is located inside the articular capsule, originates from the anterior edge of the ilium and loops around the head of the femur.
- Ligament of the femoral head - located inside the joint capsule, protecting the blood vessels of the femoral head.
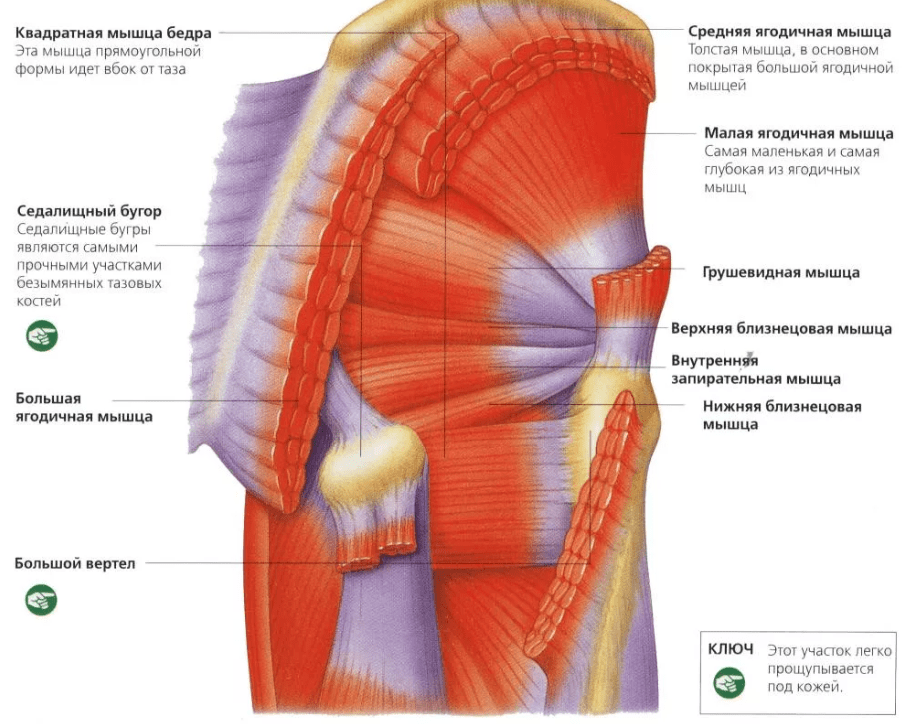
Muscles of the hip joint
The hip joint has several axes of rotation:
- frontal (transverse),
- sagittal (anterior-posterior),
- longitudinal (vertical).
 Joint movements along the frontal axis provide flexion and extension movements of the hip. The following muscles are responsible for hip flexion:
Joint movements along the frontal axis provide flexion and extension movements of the hip. The following muscles are responsible for hip flexion:
- straight,
- comb,
- ilio-lumbar,
- tailor,
- wide.
Hip extension is provided by antagonist muscles:
- two-headed
- semitendinosus,
- semimembranous,
- big buttock.
Along the sagittal axis, adducting and abducting movements of the thigh are performed. Responsible for hip abduction:
- pear-shaped
- twin,
- internal obturator muscle.
Bringing is carried out:
- big adductor,
- comb,
- thin,
- short and long adductor muscles.
 The longitudinal axis of rotation is necessary for rotation of the hip, as well as for pronation and supination of the joint. These functions are:
The longitudinal axis of rotation is necessary for rotation of the hip, as well as for pronation and supination of the joint. These functions are:
- square,
- big buttock,
- ilio-lumbar,
- pear-shaped
- twin,
- tailor,
- external and internal obturator muscles.
Blood supply of TBS
 The blood supply of the hip joint is carried out;
The blood supply of the hip joint is carried out;
- ascending branch of the lateral femoral artery
- round ligament artery,
- acetabular branch of the obturator artery,
- branches of the inferior and superior gluteal arteries,
- deep branch of the medial femoral artery
- branches of the external iliac artery
- branches of the inferior hypogastric artery.
The importance of these arteries for providing blood supply to the hip joint is not the same. The main food is provided by the deep branch of the medial femoral artery. The outflow of blood from the joint and surrounding tissues is provided by the branches of the femoral, hypogastric and iliac veins.
Innervation and lymphatic drainage of the hip joint
 The hip joint is innervated by branches of the femoral, obturator, sciatic, lower gluteal, and genital nerve trunks.
The hip joint is innervated by branches of the femoral, obturator, sciatic, lower gluteal, and genital nerve trunks.
Also, periarticular neurovascular formations and nerve roots of the periosteum take part in the innervation.
The lymphatic drainage of the joint passes through deep lymphatic vessels leading to the pelvic lymph nodes and internal sinuses.
Functions of the hip joint
One of the main functions of the hip joint is to connect the lower limbs to the body. In addition, the joint plays an important role in ensuring their movement, performing the following functions:
- supports,
- bending,
- extension,
- rotation,
- pronation,
- supination,
- leads,
- leg adduction.
Possible causes of hip pain
Daily stress, trauma, age-related changes, inflammatory and infectious processes in the tissues of the joint and its surroundings can cause pain.
Injuries
Trauma is one of the most common causes of pain in the hip area. The severity of symptoms is directly related to the severity of the injuries.
The most mild joint injury is a bruise resulting from a blow or a fall on its side. Symptoms of a bruise are pain in the thigh area, swelling and redness, temporary lameness.
 A more severe injury to the hip joint is a dislocation, which can be the result of a strong blow, for example, in a traffic accident, a fall from a height, a sharp jerk, excessive movement. Dislocation symptoms are:
A more severe injury to the hip joint is a dislocation, which can be the result of a strong blow, for example, in a traffic accident, a fall from a height, a sharp jerk, excessive movement. Dislocation symptoms are:
- sharp pain, aggravated by attempts to move the leg or lean on it;
- swelling and redness of tissues in the area of the damaged joint;
- the formation of an extensive hematoma in the thigh area;
- visually distinguishable deformities, protrusion on the thigh at the site of ligament rupture;
- forced rotational position of the limb;
- loss of functionality of the affected leg.
The most severe injury is considered to be a fracture of the femoral neck. In young and middle-aged people, such injuries are relatively rare, and occur as a result of severe blows received in a car accident or falling from a height. The vast majority of hip fractures occur in older people.
The bone tissue of the elderly loses its strength as a result of hormonal and age-related changes that accelerate the processes of calcium leaching. A fracture can occur with little physical impact or even spontaneously, in the absence of any external causes.
 Symptoms of a hip fracture:
Symptoms of a hip fracture:
- pain in the groin;
- loss of functions of the injured limb, inability to lean on it;
- forced rotational position of the leg outward;
- visually distinguishable in the prone position shortening of the injured limb relative to the healthy one;
- sticky heel syndrome - the inability to raise a leg straightened at the knee from a supine position;
- swelling and redness of tissues.
Inflammatory and degenerative diseases
One of the most common causes of pain in the hip joint are inflammatory processes in the tissues.
Arthritis- inflammation of the tissues of the joint caused by autoimmune reactions, chronic damage, bacterial or viral infections. The disease can affect both one and both joints, manifesting itself as pain that worsens after exertion and with a long stay in a motionless position, limited mobility, swelling, redness of the tissues, and local fever.
 arthrosis of the hip joint, or coxarthrosis, is a chronic, steadily progressive disease, accompanied by degenerative-dystrophic changes in tissues. The causes of development can be trauma, genetic predisposition, endocrine disorders. In the early stages, pain in the articular area is the only symptom, progressing, the disease leads to dysfunction of the joint and, ultimately, its complete destruction.
arthrosis of the hip joint, or coxarthrosis, is a chronic, steadily progressive disease, accompanied by degenerative-dystrophic changes in tissues. The causes of development can be trauma, genetic predisposition, endocrine disorders. In the early stages, pain in the articular area is the only symptom, progressing, the disease leads to dysfunction of the joint and, ultimately, its complete destruction.
Bursitis- an inflammatory process that develops in the synovial cavity of the trochanteric bag of the joint. The causes of development can be chronic injuries, as well as complications of inflammatory diseases of the joint. A characteristic symptom of the pathology is pain in the subgluteal region and on the back of the thigh, aggravated by running or walking.
Tendinitis- inflammation of the ligaments that stabilize the joint. In most cases, the cause of the development of the disease is inadequately high loads and regular microtraumas of the connective tissue. As a result of the formation of micro-tears in the fibers, scars are formed, and when pathogenic microorganisms enter them, an inflammatory process develops.
Systemic connective tissue diseases
Systemic connective tissue diseases mostly develop as a result of pathological autoimmune reactions or genetic disorders; in this case, several joints are involved in the pathological process at once.
 Gout- pathological accumulation of uric acid salts in organs and tissues, causing inflammation of the joints and the formation of tophi - specific bumps in the affected joints.
Gout- pathological accumulation of uric acid salts in organs and tissues, causing inflammation of the joints and the formation of tophi - specific bumps in the affected joints.
ankylosing spondylitis, or ankylosing spondylitis, - a genetically determined disease, in the early stages manifested by pain and a decrease in the amplitude of movements, and in the later stages - leading to ankylosis - a complete loss of mobility - of the affected joints.
epiphysiolysis- a disease based on the mechanisms of development of which are endocrine disorders, presumably of a hereditary nature. The main symptom of the pathology is the displacement and slippage of the femoral head from the acetabulum, accompanied by forced outward rotation of the limb, changes in gait, lameness and chronic pain in the hip joint.
Diagnostics
Treatment of diseases of the hip joint is impossible without making an accurate diagnosis, since there are many reasons for the development of pain syndrome and impaired mobility, and each pathology involves its own tactics and choice of treatment methods. At the initial stage of diagnosis, the specialist conducts an examination and history taking, and also prescribes a number of instrumental and laboratory tests to clarify the clinical picture:
- radiography allows you to identify the integrity of bone structures, the presence of foci of tissue changes;
- ultrasound detects changes in soft and cartilaginous tissues;
- MRI and CT help to obtain the most accurate picture of the affected area for layer-by-layer study;
- arthroscopy and examination of effusion - pathological fluid that accumulates in the synovial capsule.
Prevention of diseases and injuries of the hip joint
 Injuries and diseases of the hip joint are the most common orthopedic pathologies that can be encountered by both professional athletes and people who are as far from sports as possible. To minimize the risk of complications will allow the observance of a number of preventive measures.
Injuries and diseases of the hip joint are the most common orthopedic pathologies that can be encountered by both professional athletes and people who are as far from sports as possible. To minimize the risk of complications will allow the observance of a number of preventive measures.
The anatomy of the human hip joint (HJ) is interesting because of its significant modification over the course of evolution, which can be seen when compared with mammals that are not upright. Maintaining body weight in a vertical position required special mechanics of this joint, which cast a shadow on the structure of the joint.
The hip joint is the link between the trunk and lower limbs. It is a strong and spherical joint. Its structure is aimed at maintaining stability and performing a large number of movements in it.

Important! The hip joint is the second most mobile in the human body.
Bone anatomy - what connects and how
The head of the femur has the shape of a sphere located on the "leg" - its neck. Its entire surface is covered with articular cartilage, thickening in places of increased impact of body weight on the lower limb. An exception is the place of attachment of the own ligament of the femoral head, namely its fossa (English, fovea for the ligament of the femoral head).
The acetabulum (English, acetabulum), in turn - the second main component of the joint, is a hemisphere, covered for most of its length with cartilaginous tissue. This reduces the friction of the head on the pelvic bone.

In the photo - intra-articular surfaces - head and cavity (fossa)
The cavity is a consequence of the connection of the three bones of the pelvis - the ilium, ischium and pubis. It consists of a crescent-shaped rim, protruding somewhat upward, covered with cartilage, and being the articular part of the joint, as well as the surface of the acetabulum, which has the same shape.
Attached to the rim is an acetabular "lip" (English, acetabular labrum), which looks like a lip, due to which it got its name. By means of it, the surface area of this cavity is increased by about 10%. The part of the acetabulum that is not involved in the formation of the joint is called the fossa, and is made entirely of the ischium.
Due to the presence of a full-fledged connection between the femoral head and the pelvic bones, the structure of the hip joint allows it to remain one of the most stable joints. The congruence of the articular surfaces is most complete in the position of flexion in the joint at 90°, abduction of the lower limb by 5°, and external rotation by 10°. It is in this position that the axis of the pelvis coincides with the axis of the femoral head and forms a straight line.
Joint capsule and its ligamentous apparatus
The stability of the hip joint is further strengthened by closing this joint along its entire length with two layers of the capsule - a loose outer fibrous layer and an inner synovial membrane.

Hip ligaments are compacted parts of the fibrous layer of the capsule, which are spirally stretched between the bones of the pelvis and thigh, thereby strengthening this connection.
The structure of the human hip joint, especially its ligamentous apparatus, causes the head to completely enter the acetabulum when it is extended by rewinding the spiral ligaments that tighten the fibrous capsule, problems in this place can. Thus, the congruence of the joint during its extension is produced by passive movements of its articular surfaces.
Tensioned ligaments of the fibrous capsule limit excessive extension, which results in a lack of 10-20° to a full vertical position, however, it is this slight difference in angle that increases the stability of this joint.
The structure of the TBS includes three internal ligaments:
- Iliofemoral ligament. It is located in front and somewhat upward, stretching between the lower anterior iliac spine (English, anterior inferior iliac spine) and the intertrochanteric line of the thigh distally.
It is believed that this ligament is the strongest in the body. Her job is to limit hyperextension of the hip joint in a standing position. - pubofemoral ligament(English, pubofemoral ligament). It extends from the obturator crest, heading down and laterally to the connection with the fibrous capsule. Intertwined with the medial part of the iliofemoral ligament, it also participates in limiting excessive extension of the joint, but to a greater extent prevents hip hyperabduction (too much abduction).
- Ischiofemoral ligament. Localized on the back surface of the joint. It is the weakest of all three ligaments. Spiral around the neck of the femur, attaching to the base of the greater trochanter.

An important role in gait is played by the hip joint, the structure of which is maintained precisely thanks to the above-described ligaments and the muscular skeleton, which ensure its structural integrity. Their work is interconnected, where the lack of some elements is covered by the advantage of others. Learn more about this in the video in this article.
Thus, the work of the ligamentous and muscular apparatus is balanced. The medial hip flexors, located anteriorly, are weaker than its medial rotators, but their function is enhanced by the anterior internal thigh ligaments (pubofemoral and iliofemoral), which are much stronger and denser than the posterior ligament of the joint.
The only ligament that performs almost no function in relation to strengthening the joint is the ligament of the femoral head. Its weak fibers are directed from the fossa, located in the center of the femoral head, to the acetabular notch. Her job is mostly to protect the vessel (artery of the femoral head) that runs between her fibers.
The fatty tissue that fills the fossa of the acetabulum, together with the ligament, is covered with a synovial membrane. This adipose tissue compensates for the lack of congruence of the articular surfaces by changing its shape during movements.
Movements in the joint
It:
- flexion and extension;
- abduction and adduction;
- medial and lateral rotation;
- rotation.
All of the above movements are extremely important, as they provide such daily human activities as getting out of bed, keeping the body upright, sitting, if you have problems with the implementation of these simple actions, check out.
The anatomy of the hip joint is rich in muscles that allow the implementation of the above-described functions of the hip joint.
These include:
- iliopsoas muscle (eng., iliopsoas muscle) - the strongest flexor of the lower limb;
- the large adductor muscle is its synergist;
- simultaneous flexion and adduction of the limb is provided by the piriformis and gracilis muscles;
- the small and middle gluteal muscles serve simultaneously as abductor and medal rotators;
- the gluteus maximus plays the role of the main extensor, participating in the transition of the body from a bent position in the hip joint to an extended one (standing up).
blood supply
The head and neck of the femur are supplied by branches of the medial and lateral circumflex arteries, the deep femoral artery, and the own artery of the femoral head. In adulthood, the medial circumflex femoral artery is considered the most important source of blood supply to the femoral head and proximal part of its neck.
Attention! In old age, the blood supply to the head and proximal part of the femoral neck decreases, which leads to a high incidence of trauma in this area and difficulty in healing fractures, which often requires a complete or partial replacement of the joint to restore its mobility.

Among other things, recovery after a hip fracture is lengthy and requires patience and the desire of the patient, but more importantly, the full implementation of all the techniques that the instructions developed by the rehabilitation doctor offer. The lesson plan is developed individually and requires the efforts of the patient.
Important! Only a doctor can diagnose problems in TBS and prescribe the appropriate treatment. If symptoms appear that indicate a violation of full-fledged movements in this joint, contact an orthopedist-traumatologist.
Go to the contents of the Bulletin of the RNCRR of the Ministry of Health of the Russian Federation N8.
Current section: Imaging
Modern data on the anatomy and blood supply of the hip joint, clinic and diagnosis of its inflammatory-necrotic lesions.
Khisametdinova G.R., Federal State Institution “RNTSRR Rosmedtechnologii” Moscow.
The main task of early diagnosis of Perthes disease, aseptic necrosis of the femoral head of another genesis, is to detect the stage of vascular disorders, when, if adequate measures are taken, the process can reverse. Ultrasound with Doppler ultrasound, which allows assessing regional blood supply in various pathologies of the hip joints in children, is an important method for assessing the effectiveness and adequacy of the treatment, load regulation and functional therapy.
Key words: hip joint, diagnostics, blood supply Khisametdinova G. R.
The modern knowledge about the anatomy and blood supply of the hip joint in clinics and diagnostics of its inflammatory-necrotic lesions
Federal State Enterprise Russian Scientific Center of Roentgenoradiology (Russian Medical Technologies Department)
The main purpose of the early diagnostics of Pertes’ disease and of other hip bone aseptic necrosis is the detection of their vascular stage, when adequate therapy may cause resolution of the disease. Sonographic investigation with Doppler techniques assesses regional blood supply in different pathology of hip joint in children, and evaluates the effectiveness and adequacy of the treatment to adjust load and functional therapy.
Keywords: hip joint, diagnostics, blood supply
Etiology, classification and clinic of Legg-Calve-Perthes disease and aseptic
necrosis of the femoral head of another origin.
Ultrasonic methods for studying the hemodynamics of the hip joint. Ultrasonic research methods for a number of pathologies of the hip joint. Bibliography.
Embryogenesis, anatomy and blood supply of the hip joint.
The hip joint is the largest human joint. Of considerable interest is the embryogenesis of the hip joint in terms of substantiating the congenital predisposition to various pathological conditions. In a number of diseases of the hip joint, which are detected in young children, there is a single mechanism of violation of embryogenesis during the laying of the musculoskeletal system, which leads, in the process of growth and formation of the musculoskeletal structures of the hip joint, to a violation of their spatial relationship.
All elements of the hip joint are formed from a single scleroblastoma mass. The skin and its derivatives develop from the ectodermal layer, cartilage, bones, tendons, ligaments and a capsule develop from the mesodermal layer. Already at the end of the 4th week of gestation, the rudiments of the lower extremities in the form of vascularized mesenchymal nuclei are determined in the embryo. Between the 6th and 7th weeks, the first cartilaginous elements appear, and in the hip joint, 3 cartilaginous elements of the thigh unite into a cartilaginous formation (“hemitase-semipelvis”) and create a flat acetabulum. Between the acetabulum and the cartilaginous elements of the thigh, the future joint space is still made of connective tissue. At this stage, the cartilaginous lip is already recognized as dense connective tissue.
At the 7th week of intrauterine development, when the embryo is about 1 cm long, the articular cavity, ligament of the femoral head, joint capsule and joint space appear (Fig. 1). The femoral diaphysis ossifies, and the bone tube of the diaphysis and the medullary space appear. Bone anlages are formed from precartilaginous cells. By this time, the arterial trunks have already been formed and the nerves - femoral and sciatic - have been delimited. The future joint cavity is defined as a zone of dense cells between the femoral head and the pelvis. The precartilaginous cells atrophy during the formation of the joint and, in the process of autolysis, the joint space, the spherical head of the femur and the semicircular articular cavity are formed from the primitive cavity of the joint. On the upper border of the cavity, a limbus is defined in the form of a wedge-shaped edge, along the edge
cartilaginous iliac bone, a fibrocartilaginous rim is noticeable - the future labrill acelabullage.
At the end of the 8th week, the initial development of the hip joint is almost completed. The pelvis is formed by ossification of three components, each of which has its own nucleus. The first nucleus of ossification occurs in the body of the ilium at week 10.
The fetus of 11-12 weeks has a length of about 5 cm, the hip joint of which is formed with all structures, calcification of the diaphysis ends.
At 16 weeks, the fetus is 10 cm long, the head of the femur is spherical, 4 mm in diameter, all movements in the hip joint are possible, and the nucleus of the ischium is ossified.
By the 20th week, all differentiation is completed, the ilium is ossified by 75%, the core of the pubic bone is ossified, while the bone formations are united by a Y-shaped cartilage, the femoral head is 7 mm in diameter, remains cartilaginous up to 3-4 months after birth.
Rice. 1 Planar section of the hip joint of a 7-week-old embryo
The anatomical structure of the hip joint in young children is significantly different from that of an adult. Features of the hip joint of newborns are that the predominant part of the elements of the joint in the process of its development is cartilaginous. One center of ossification is located in the nucleus of the epiphysis of the femoral head, and the second is in the nucleus of the greater trochanter. The nucleus of the epiphysis of the femoral head appears in the period from the 2nd to the 8th months of life, the nucleus of the greater trochanter - between the 2nd and 7th years of life. Ossification of the femoral head is carried out from two sources: due to the ossification nucleus of the proximal femoral epiphysis, and also due to
the spread of the process of enchondral bone formation from the side of the zone of ossification of the femoral neck in the proximal direction. The upper-inner section of the femoral head is ossified from the ossification nucleus of the proximal epiphysis of the femur, and the lower-outer section is from the zone of ossification of the femoral neck.
In the first year, the degree of ossification of the femoral neck increases, the cartilaginous structure retains only its upper section. The greatest growth rates of the acetabulum are observed in the first year of life and in adolescence. The cavity diameter increases due to the growth of the Y-shaped cartilage. The depth increases due to the growth of the cartilaginous edges and the acetabular lip, as well as due to its physiological protrusion in older children. The most active deepening of the acetabulum occurs from 2 to 3 years and after 5 years of age. The growth of the femoral head occurs synchronously with the growth of the acetabulum, while the highest rate of its ossification is observed from 1 year to 3 years.
The data on the anatomy of the hip joint presented in the review, its blood supply, make it possible to explain the pathogenesis, symptoms of the development of clinically different forms of hip joint pathology.
The hip joint is a type of ball-and-socket joint of a limited type - a cup-shaped joint. Movements are performed in three planes: frontal (abduction up to 135 degrees, adduction up to 60 degrees), sagittal (flexion up to 40 degrees, extension up to 10 degrees) and vertical (outward rotation up to 41 degrees, inward rotation up to 35 degrees), as well as circular movement. The stability of the joint is ensured by the anatomical shape of the articular ends, the joint capsule, powerful ligaments and muscles.
The joint is formed by the proximal end of the femur, the articular surface of the head, as well as the bones of the acetabulum, which consists of the ilium (upper section), ischial (lower-posterior section) and pubic (antero-internal section) bones (Fig. 2.3). In children, these bones are separated from one another by a Y-shaped growth cartilage. By the age of 16, the cartilage ossifies, and individual bones, growing together, form the pelvic bone. The acetabulum is covered with cartilage only in the region of the lunate surface, the rest of it is filled with fatty tissue and covered with a synovial membrane. The thickness of the cartilage is from 0.5 to 3 mm, it reaches its greatest thickness in the zone of maximum load. A fibrocartilaginous acetabular lip is attached along the free edge of the cavity, which increases the depth of the acetabulum.
Scheme of the frontal cut of the right hip joint
1. wing of the ilium;
2. iliac muscle;
3. small gluteal muscle;
4. gluteus medius; acetabulum;
5. gluteus maximus;
6. acetabulum; the border
7. acetabular (cartilaginous) lip; hips;
8. circular zone; preparations
9. femoral head; hollows;
1. bone protrusion (bay window);
2. perichondrium and periosteum of the ilium;
3. cartilaginous lip
4. big skewer;
5. osteocartilaginous
proximal part
6. acetabular fossa isolated in the process
Anatomical preparation of a cut of a child's hip joint, corresponding to Fig. 2
10. large skewer;
7. Dedicated in progress
preparations
II. swivel bag large
8. cartilaginous part of the roof
gluteal muscle;
12. articular capsule with a circular zone;
13. iliopsoas muscle;
acetabulum;
9. periosteum internal
pelvic walls.
14. medial artery enveloping the thigh;
15. comb muscle;
16. perforating arteries.
The head of the femur is covered with hyaline cartilage throughout, with the exception of the fovea capitis, where the ligament of the head is attached, in the thickness of which the vessels pass to the head of the femur.
The articular bag connects and covers the articular ends of the bones, forming a cavity of the hip joint, consisting of the cervical region and the acetabulum, which communicate with each other. In the joint capsule, the outer fibrous layer, reinforced by ligaments, and the inner synovial layer, lining the joint cavity, are distinguished. The fibrous capsule is attached to the pelvic bone along the edge of the acetabular lip, on the femur it is fixed along the intertrochanteric line, and from behind captures 2/3 of the femoral neck.
The articular bag is reinforced with ligaments: three longitudinal (in front - ilio-femoral and pubic-femoral, behind - ischio-femoral) and circular, running in the deep layers of the joint capsule.
The hip joint has two intra-articular ligaments: the aforementioned ligament of the head, covered with a synovial membrane and the transverse ligament of the acetabulum, which in the form of a bridge is thrown over the opening of the acetabulum. The muscles that provide movement in the hip joint include the muscles of the pelvis and the muscles of the free lower limb. The muscles of the pelvis are divided into muscles starting in its cavity (large and small lumbar, iliac, piriformis, coccygeal, internal obturator) and muscles starting on the outer surface of the pelvis (tensor fascia lata, large, middle and small gluteal, upper and lower twin , rectus and quadratus femoris). The hip joint has three sources of innervation. It is innervated by branches of nerves: in front - femoral, medial - obturator and behind - sciatic. Due to
features of innervation, with pathology of the hip joint (Perthes disease, coxitis), pain often radiates to the knee joint.
Rice. 4 Blood supply to the hip joint
1. deep artery enveloping the ilium;
2. superficial artery enveloping the ilium;
3. femoral artery;
4. ascending branch of the lateral circumflex artery of the thigh;
5. transverse branch of the lateral circumflex artery of the thigh;
6. descending branch of the lateral circumflex artery of the thigh;
7. lateral circumflex artery of the thigh;
8. deep femoral artery;
9. perforating arteries;
10. external iliac artery;
11. inferior epigastric artery;
12. superficial epigastric artery;
13. superficial external pudendal artery
14. obturator artery;
15. deep external genital artery;
16. medial circumflex artery of the thigh;
17. femoral artery;
18. muscular branches.
Of great importance in the normal development and functioning of the hip joint is its blood supply (Fig. 4). The main role in the blood supply of the joint belongs to the medial and lateral arteries that go around the femur (branches of the deep femoral artery) and the obturator artery. The remaining supply vessels are involved in the blood supply of the proximal femur through anastomoses with the three listed arteries.
Normally, there are several types of structure of the arterial network: the medial and lateral arteries enveloping the thigh can depart from the deep femoral artery, directly from the femoral artery, from a.comitans n.ischiadici.
The deep artery of the thigh, is the main vessel through which the vascularization of the thigh is carried out, it is a thick trunk that departs from the posterior side of the femoral artery (a branch of the external iliac artery) 4-5 cm below the inguinal ligament, lies first behind the femoral artery, then appears from the lateral side and gives off numerous branches, including:
1. the medial artery that surrounds the femur, a.circumflexa femoris medialis, which departs from the deep artery of the thigh behind the femoral artery, goes transversely inward and, penetrating between the iliopsoas and pectineus muscles into the thickness of the muscles that bring the thigh, bends around the neck from the medial side femur, gives the following branches:
a) ascending branch, r. ascendens, is a small stem that goes up and inwards, branching out, approaches the comb muscle and the proximal part of the adductor longus muscle.
b) the transverse branch, r.transversus, is a thin stem, goes down and medially along the surface of the pectinus muscle and, penetrating between it and the long adductor muscle, goes between the long and short adductor muscles. Blood supply to the long and short adductor muscles, thin and external obturator muscles;
c) deep branch, r. profundus, a larger trunk, which is a continuation of the medial circumflex artery of the thigh. It goes backwards, passes between the obturator externus muscle and the square muscle of the thigh, dividing here into ascending and descending branches (superior and inferior cervical arteries);
d) branch of the acetabulum, r. acetabularis, a thin artery, anastomoses with branches of other arteries that supply the hip joint.
2. lateral circumflex artery of the femur, a. circumflexa femoris lateralis, large trunk, departs slightly below the medial, from the outer wall of the deep
arteries of the thigh almost at its very beginning, goes to the lateral side. It goes outward in front of the iliopsoas muscle, behind the sartorius muscle and the rectus femoris, approaching the greater trochanter of the femur, is divided into branches:
a) the ascending branch, r. absepense, goes up and outward, lying under the muscle that stretches the fascia lata and the gluteus medius muscle;
b) the descending branch, r.deBsepeenF, is more powerful than the previous one. It departs from the outer surface of the main trunk and lies under the rectus femoris muscle, then descends along the groove between the intermediate and lateral wide muscles of the thigh, supplying them with blood, the quadriceps femoris muscle and the skin of the thigh.
c) the transverse branch, r. lxan8veere8, is a small stem, directed laterally; supplies the proximal rectus femoris and vastus lateralis muscles of the thigh.
Branches of the lateral circumflex artery supply the superficial portion of the anterior segment of the head and neck of the femur.
The main age-related feature of the blood supply in children is the autonomy and disunity of the vascular system of the epiphysis and the femoral neck. The barrier between them is the growth zone, which prevents the vessels supplying the distal femur and the hip joint capsule from penetrating into the head of the femur.
The medial circumflex artery of the thigh gives off two branches: the superior cervical artery and the inferior cervical artery. The superior cervical artery supplies most of the epiphysis of the femoral head (from 2/3 to 4/5). It penetrates the epiphysis from the outside, forms a dense network of vessels at its base, supplying the reserve layer of cells of the growth plate with blood. The anterior central region of the epiphysis is located in the terminal zone of the vascular basin of the superior cervical artery, that is, it is located in the least favorable zone of blood supply. The inferior cervical artery only supplies the small medial segment of the head.
The obturator artery, is a branch of the internal iliac artery, it feeds the obturator externus muscle, adductors and gives rise to the acetabular branch, which penetrates through the opening of the acetabulum into the hip joint and nourishes the ligament of the femoral head and the head of the femur.
The arteries of the ligament of the femoral head originate from two sources - the obturator and medial circumflex artery. The thinnest arteries of the ligament of the head branch out in a loose and main type. In the first case, the arteries usually do not penetrate into the femoral head, in the second, they spread in it to a limited extent.
plot. In children, there are no anastomoses between the branches of the superior and inferior cervical arteries and the arteries of the ligament of the femoral head. Arterial anastomoses occur at an older age.
Vessel branches form Anserov's annular arterial anastomosis along the edge of the cartilaginous cover of the femoral head (Fig. 5). Thanks to the anastomosis, more uniform nutrition of the individual segments of the head is carried out. The second arterial ring is formed by the medial and lateral arteries that go around the thigh. Damage to the arteries that occurs below this anastomosis can lead to serious changes in the area of blood supply to this vessel. Therefore, both traumatic and hemodynamic disorders of the vascular network of the capsule of the hip joint can lead to impaired blood supply to the epiphysis of the femoral head, which leads to the occurrence of aseptic necrosis and destruction of the bone structure. Due to the absence of anastomoses that occur only after 15-18 years, after synostosis of the head and neck of the femur, any traumatic effect on the hip joint (especially trauma, cooling, vascular spasm, etc.) can remain invisible under equal conditions in adults and cause complications in children.
Rice. 5 Arterial anastomoses of the femoral head
The venous system differs from the arterial system in its architectonics. In the wide bony canals of the neck, one artery is accompanied by two or more venous trunks. The veins emerging from the epiphysis of the femur anastomose with the veins of the articular capsule, and
also with the veins of the muscles surrounding the joint. Venous outflow from the hip joint occurs from the intraosseous plexuses through the medially and laterally surrounding the thigh veins into the deep femoral vein, femoral vein, external iliac vein.
Etiology, classification and clinic of Legg-Calve-Perthes disease and aseptic necrosis of the femoral head of another origin.
Legg-Calve-Perthes disease is an osteochondropathy morphologically and pathophysiologically, which is aseptic necrosis of the bone tissue of the femoral head and its secondary deformation due to axial load. It is reliably known that osteonecrosis develops as a result of a violation of the local vascular, namely, arterial nutrition of the bone substance and bone marrow.
Up to 30 synonyms of osteochondropathy of the femoral head are known, in which the authors tried to reflect both the morphological substrate and the etiological moment in the development of the disease. The most common terms for pathology are: Perthes disease, aseptic necrosis of the femoral head, coxa plana.
For the first time, almost simultaneously, independently of each other, this pathology was described by the orthopedists Waldenstrum in 1909 and Legg, Calve and Perthes in 1910.
According to the Ministry of Health of the Russian Federation, in the structure of disability due to injuries and diseases of the musculoskeletal system, osteochondropathy accounts for 27%, which is 2% more than disability due to injuries. Among all osteochondropathy, Perthes' disease is, according to different authors, from 3 to 13%. Most often, Perthes disease affects children aged 4 to 10 years, but cases of the disease at an earlier and especially at a later age up to 18-19 years are not uncommon. Boys and young men are affected 4-5 times more often than girls.
In most cases, the process is unilateral, but there is also a bilateral lesion, which develops not simultaneously, but sequentially one after another for 6-12 months. Bilateral lesion, according to different authors, is noted in 7-20%. Among orthopedic diseases of the postnatal period, congenital hip dislocation attracts the most attention due to its prevalence and the most common cause of disability in children and adolescents. The frequency of congenital dislocation of the hip in all countries and regions, regardless of race, averages from 2 to 3%, in unfavorable regions up to 20%. According to Ya.B. Kutsenko et al (1992), congenital dysplasia, subluxation and dislocation of the hip occur in 5.3 cases per 1000 newborns. Congenital dislocation of the hip occurs predominantly in girls in a ratio of 1:5, left-sided dislocation occurs twice as often as right-sided. The probability of having a child with congenital hip dislocation increases with breech presentation, with a positive family history, with other congenital deformities, with congenital pathology of the neuromuscular apparatus (Spina bifida, cerebral palsy, etc.). Violation of the blood supply to the bone tissue is due to both congenital underdevelopment of the vascular bed in the area of the hip joint, and the trauma of modern operations to reduce the dislocation (osteotomy of the femur, pelvic bones, etc.).
According to some authors, aseptic necrosis of the femoral head develops in 10-50% of patients with various injuries of the hip joint area in the immediate or long term after the injury. Its most common causes are surgical interventions in this region that were transferred in childhood, bruises in the area of the hip joint, a fracture of the femoral neck, and traumatic dislocation. The collapse of the femoral head is determined within a period of six months to three years from the moment of injury and is associated with a functional load on the pathologically altered head.
If the causes of the development of aseptic necrosis of the femoral head are severe orthopedic diseases (congenital dislocation of the hip, osteomyelitis of the femur, etc.), then the causes of the development of Perthes disease have not been fully disclosed to date. The vast majority of orthopedists now believe that the pathogenesis of degenerative-dystrophic diseases of the hip joint is a violation of its blood supply or ischemia. There are several views regarding the nature of vascular disorders leading to the development of aseptic necrosis of the femoral head:
Repeated heart attacks due to arterial thrombosis;
Latent prolonged insufficiency of arterial blood supply;
Venous stasis;
A combination of disorders from both the arterial and venous networks.
As factors causing these pathological conditions, as well as contributing to their occurrence, are called:
Congenital hypoplasia of the vessels of the femoral head;
Violations of the neurovascular mechanisms;
Anatomical and functional features of the blood supply to the hip joint in childhood, due to insufficient vascularization of the femoral head associated with the anatomical and functional immaturity of the vascular network;
3) retardation of the development of the retinacular vessels of the femoral neck from the growth of secondary centers of ossification;
4) asynchrony in the development of the medial and lateral circumflex arteries of the thigh, which contributes to the appearance of a shortage of blood supply to the femoral head. These data indicate that in children under 8 years of age, due to imperfect blood circulation in the proximal femur, there is a potential possibility, under certain unfavorable conditions, of the occurrence of aseptic necrosis of the femoral head or Perthes' disease. The head of the femur during this period of a child's life can be characterized as locus minoris resistentiae.
A number of authors, using angiographic and radioisotope studies of blood flow, indisputably established the presence of spasm of the main vessels and vessels of the second and third order, as well as a decrease in mineral metabolism on the side of the disease.
G. A. Ilizarov (2002) proposed a general biological theory called “about the adequacy of vascular nutrition and the motor function of a limb or its segment.” For the normal functioning of the bone tissue of the musculoskeletal
apparatus must be in full compliance with vascular nutrition and function. For example, if for some reason vascular nutrition is reduced in a given area of bone tissue, and motor function is enhanced, then tissue destruction is inevitable.
G.I. Ovchinnikov (1991), on the basis of phlebographic studies, concludes that in aseptic necrosis due to discoordinated vascular spasm-paresis, a pathological type of blood circulation develops, leading to the discharge of incoming arterial blood into the diaphyseal venous system of the thigh, and the tissues of the femoral head are in a state of chronic ischemia. Under these conditions, demineralized bone trabeculae undergoing further resorption break down and are impressed. And since the pathogenetic basis of the disease is ischemia, instead of strengthening the reparative processes, they are suppressed.
M.G. Weight gain (1938) showed that the arteries of the femoral head are terminal, and therefore such a mechanism for the development of aseptic necrosis of the femoral head as thromboembolism deserves attention. The very fact of blockage of blood vessels can be considered in the acute onset of the disease in some patients.
The form of the lesion of the femoral head, according to O.V. Dolnitsky, A. A. Radomsky (1991), depend on an isolated or general blockade of certain vessels that feed the epiphysis. They put forward the concept of blockade of the vascular pools of the femoral head in Perthes disease, which consists in the defeat of the nominal area of the head that the vessel fed before blocking, that is, if the upper cervical artery, which feeds 2/3 of the ossification nucleus, and the lower cervical artery, are blocked, then there is a total variant of the defeat of the femoral head. Therefore, depending on the topography and the degree of blockade of the arteries and their branches that feed the femoral head, subchondral, medial, limited, subtotal and total lesions occur. There is evidence of circulatory disorders in the joint capsule and changes in the biochemical composition of the synovial fluid.
A significant place in the pathogenesis of Perthes disease, as a triggering factor, is given to trauma. S.A. Reinberg (1964) put forward a hypothesis about a violation in Perthes' disease of the sympathetic innervation of the intraosseous vessels of the head, which leads to a spasm of the vessels that feed the bone structures. This was reflected in the works of Chuchkov V.M. (1990).
According to Yu.A. Veselovsky (1989), the spasm of the vessels supplying the femoral head is based on a dysfunction of the vegetative ganglia of the lumbar -
sacral spine and spinal centers at the level of TTL-BT. Dysfunction of the autonomic nervous system is predominantly of ganglion-sympathetic origin and manifests itself in the prevalence of sympathotonus with anatomical and functional immaturity of the vascular network. This complex leads to ischemia of the proximal femur and aseptic necrosis of the femoral head. Thus, a combination of factors plays an important role in the development of aseptic necrosis of the femoral head, including both neurovascular disorders, a special hormonal background, environmental influences, and structural features of the hip joint in biomechanical terms.
The restructuring process underlying any changes in the shape and structure of the bone depends not only on the state of the blood supply, but also on the conditions of the functional load. These two factors together lead to the activation of bone remodeling processes, which can occur with a predominance of both osteogenesis over resorption and resorption processes over bone formation.
It should be recognized that aseptic necrosis of the femoral head is a polyetiological disease, the initial trigger of which is associated with microcirculatory homeostasis disorders, possibly against the background of anatomical and functional inferiority of the hip joint caused by endogenous and exogenous causes. Regardless of the etiology, the pathological picture of all types of aseptic necrosis of the femoral head is similar.
The pathogenesis of Perthes disease has been established quite consistently. The disease has a staged course. Currently, 20 variants of its classification have been proposed. All options are based on the principle of systematized clinical, morphological and pathomorphological signs. The classifications of a number of modern researchers take into account, in addition, the degree of neurotrophic disorders that, in their opinion, underlie the pathogenesis of osteochondropathy. The pathological and histological changes occurring in the epiphyseal head of the femur are based on the so-called primary aseptic subchondral epiphyseonecrosis. The generally accepted classification of osteochondropathy of the femoral head was proposed by Akhausen in 1928. During the course of the disease, he distinguishes five stages.
In the first stage, the stage of necrosis, necrosis of the spongy bone and bone marrow of the epiphyseal head occurs, the bone skeleton of the head loses its normal mechanical properties, only the cartilaginous cover of the head does not die. Significant physical and chemical changes occur in dead bone tissue, mainly
in collagen fibrils, on which the strength and elasticity of bone beams depend. Despite the duration of this stage of about 6 months, according to Reinberg (1964), it does not manifest itself radiographically.
The second stage, the stage of an impression fracture and pronounced osteochondritis, is due to the resorption of dead trabeculae and the weakening of their supporting functions. The femoral head loses its ability to withstand normal loads, a depressed or impression subchondral fracture of the necrotic head occurs, the bone beams wedged into each other, are compressed, the head is flattened from top to bottom, the hyaline cartilage thickens.
The third stage, the stage of resorption, bone fragments are slowly resorbed by the surrounding healthy tissues, connective tissue strands from the femoral neck penetrate deep into the dead epiphysis, cartilage islands penetrate from the hyaline cartilage into the head, necrotic masses are surrounded by osteoclastic shafts. Due to the penetration into the head of connective tissue and cartilaginous elements with newly formed vessels, the continuity of the subchondral plate and epiphyseal cartilage is disrupted. The femoral neck is shortened due to a violation of its endochondral growth. The support function at this stage is significantly impaired. The stage is long, the course of the process is torpid, from 1.5 to 2.5 years. The fourth stage is the stage of reparation, the restoration of cartilage and bone tissue, the restructuring of the specific beam structure of the bone tissue and the femoral head, and its adaptation to new biomechanical conditions take place. Following resorption and almost simultaneously with it, the formation of new bone tissue occurs, the reconstruction of the spongy bone substance of the head occurs due to connective tissue and cartilage elements, they metaplastically turn into bone tissue. The terms of this stage are significant - 6-18 or more months. In the studies of E.A. Abalmasova (1983), Axbane O. (1928) notes that regeneration can occur without the phase of fragmentation, although S. A. Reinberg (1964) believes that the reparative process must consistently go through all phases of restructuring.
The fifth stage, the final one, has two outcomes: recovery or development of deforming coxarthrosis. Complete recovery of the femoral head occurs with the normal reverse development of dystrophic processes in the hip joint with the restoration of its normal structure and biomechanics. Deforming arthrosis occurs as a result of reactive processes in the tissue to severe changes in the trophism and biomechanics of the joint.
As a rule, the femoral head is always deformed and significantly enlarged, but ankylosis is never observed in patients, since the articular cartilage is not affected.
fully. Together with changes in the head, flattening of the acetabulum occurs again as a compensatory reaction of the bone and cartilage tissue to restore the congruence of the articular surfaces.
Not all authors adhere to this five-stage classification; three-phase, two-phase division, and others have been proposed. What all classifications have in common is that they reflect the phases of the course of the disease: necrosis, reparative regeneration and outcome.
In recent years, some authors are trying to get away from a purely anatomical and morphological interpretation of this pathology and present classifications taking into account the degree of neurotrophic disorders that, in their opinion, underlie the pathogenesis of osteochondropathy. One such classification is presented by Veselovsky et al. (1988) .
T. Initial stage - compensated latent ischemia of the proximal end of the femur:
a) without pronounced radiological changes;
b) delayed growth of the ossification nucleus of the epiphysis of the femoral head;
c) local osteoporosis of the outer parts of the head and neck of the femur.
TT. Stage of osteonecrosis - decompensated ischemia of the proximal end of the femur:
a) changes in the structure of the bone tissue of the metaphysis;
b) changes in the structure of the bone tissue of the epiphysis;
c) change in the structure of the bone tissue of the metaepiphysis.
TTT. Impression fracture stage:
a) without changing the shape of the epiphysis;
b) with a change in the shape of the epiphysis;
THAT. Fragmentation stage:
a) without changing the shape of the epiphysis and the spatial orientation of the femoral neck;
U. Stage of recovery:
b) with a change in the shape of the epiphysis or the spatial orientation of the femoral neck (but without the state of external subluxation of the head);
c) with a change in the shape of the epiphysis or the spatial orientation of the femoral neck and the state of external subluxation of the head.
UT. Exit stage:
a) without changing the shape of the epiphysis or the spatial orientation of the femoral neck;
b) with a change in the shape of the epiphysis or the spatial orientation of the femoral neck (but without the state of external subluxation of the head);
c) with a change in the shape of the epiphysis or the spatial orientation of the femoral neck and the state of external subluxation of the head.
d) with symptoms of coxarthrosis.
In T and TT stages of the lesion according to Cayega1, / of the epiphysis of the femoral head suffers, the determining factor is the presence of an intact edge of the epiphysis, which serves as a supporting column and reduces the possibility of flattening the head with subsequent deformation. In TTT and TU stages according to Sayega1, when more than / of the femoral head is affected, an unfavorable symptom is damage to the outer edge of the epiphysis of the femoral head. This increases the likelihood of flattening the head and its subsequent deformation.
Osteochondropathy of the femoral head develops in children who are quite healthy from a general clinical point of view, normally developed, in whose anamnesis there are no indications of trauma. With aseptic necrosis of the femoral head, there are indications of bruises of the hip joint, surgical interventions for hip dislocation, and osteomyelitis in the anamnesis. The disease begins gradually, with indefinite pulling pains in the hip or knee joint, along the muscles of the lower extremities. Less commonly, the disease begins acutely, when stepping, lifting weights or awkward movements, sharp pains occur that temporarily immobilize the patient. In the future, the pain syndrome becomes unstable - it appears or intensifies by the end of the day, after a long walk, it stops at rest. The pain may radiate to the hip or knee. The child begins to limp and slightly drag the injured leg. Objectively, the absence of atrophy of the affected limb or its insignificant degree is determined. Characteristic clinical symptoms are limited abduction and extension with normally preserved flexion in the hip joint, difficulty inward rotation, a positive Trendelenburg sign, and flattening of the buttock. In the future, limitation of mobility progresses, contractures develop, a “duck gait”, muscle atrophy and shortening of the limb appear. General condition and laboratory parameters
do not change significantly. The disease has a relatively benign, chronic, slow course. Healing occurs on average after 4-4.5 years. The prognosis and outcome of Perthes disease depend primarily on the timing of the start of treatment. Meanwhile, only in 6-8% of all patients, the diagnosis is established at its first stage, when the first complaints and clinical signs appear, but radiographic signs of damage to the femoral head are absent or not convincing enough. For the rest, the correct diagnosis is made only in the TTT-TTT stages, and in some cases - in the TU stage. Early diagnosis requires special research methods, since traditional radiography allows you to establish a diagnosis only in the second stage of the disease. Early diagnosis and timely treatment are the most important and determining factor in the favorable outcome of the pathological process. In the outcome of Perthes disease with timely and correct treatment, there is a complete restoration of the bone structure and shape of the femoral head, with untimely (in the late stages - TTT, TU) - a significant deformity of the femoral head and articular cavity develops.
Aseptic necrosis after closed and open elimination of congenital hip dislocation proceeds similarly to Perthes disease, but is characterized by a longer course, bone restructuring of the adjacent femoral neck.
On the basis of epiphyseal dysplasia, aseptic necrosis of the femoral head is characterized, as a rule, by a bilateral lesion, a longer course. As a result, a complete restoration of the structure and shape of the femoral head usually does not occur. Significant deformation of the head and articular cavity, pronounced violations of the ratio of articular surfaces lead to the early development of severe deforming coxarthrosis.
Post-traumatic aseptic necrosis of the femoral head occurs in 3 variants:
1) in young children - according to the type of Perthes disease with a total lesion of the femoral head;
2) in older children and adolescents - according to the type of limited necrosis of the femoral head;
3) in older children and adolescents - with the simultaneous development of necrosis of the femoral head and deforming coxarthrosis.
Thus, the analysis of the literature on aseptic necrosis of the femoral head does not give an idea of a specific etiological factor,
causing subchondral osteonecrosis of the femoral head. Therefore, one of the tasks in the performance of the work is to study the blood supply to the femoral head in aseptic necrosis to clarify the nature of this disease, which in the future can become a theoretical foundation on which a diagnostic and treatment algorithm will be built. The task of early diagnosis, in the context of modern views on the etiopathogenesis of aseptic necrosis of the femoral head, is to detect the stage of vascular disorders, when, if adequate measures are taken, the process can reverse. At the beginning of treatment in the TTT and TU stages, the prognosis is less favorable than in the T and TT stages, when it is necessary to take more effective unloading of the hip joint.
Methods for diagnosing blood flow in the vessels of the hip joint.
Perthes disease and aseptic necrosis of the femoral head of another origin occupy a special place in the group of avascular lesions of the hip joint in children, since they often develop joint deformity with impaired function. According to modern concepts, this pathology is based on a circulatory disorder in the form of a prolonged spasm of the vessels of the hip joint, leading to the appearance of foci of necrosis in the femoral head.
The number of identified patients in the first stage of Perthes disease and aseptic necrosis of the femoral head, according to leading clinics, does not exceed 10%. Therefore, the efforts of orthopedists are aimed at finding methods and ways of early diagnosis of this disease. For this, methods of contrast radiography of the vessels of the hip joints, both arterial and venous, are used, which is diagnostically significant, since the overwhelming number of orthopedists recognize the ischemic factor as leading in the pathogenesis of the disease.
Serial angiography is used to examine the arterial system in Perthes disease and aseptic necrosis of the femoral head. The examination is carried out under general or local (depending on age) anesthesia, anesthesia is first performed at the site of arterial puncture in order to prevent segmental spasm. Usually, a femoral artery puncture is used, angiographic examination is performed in a special X-ray operating room. As a contrast, a 3-iodine preparation is used - urotrast 50%. A series of angiograms consists of 9-10 shots.
Analysis of angiograms makes it possible to measure symmetrical sections of the common and internal iliac, superior and inferior gluteal arteries, the common trunk of the epigastric and obturator arteries, the lateral and medial circumflex femoral arteries on the healthy and diseased sides. Comparison of the diameter of the altered vessels on the healthy and diseased side reveals a decrease in them on the affected side, a decrease in the size of the total basin on the side of the diseased hip joint. When predicting the outcomes of the disease and choosing methods of treatment, the development of blood vessels is of decisive importance: with hypoplasia, conservative treatment is carried out, with aplasia, surgical treatment is already in the TT stage of the disease.
The most informative objective data were obtained by measuring intraosseous blood pressure in the femoral neck and transosseous contrast phlebography. In the affected joint, intraosseous pressure is sharply increased from 1567 to 4113 Pa against the norm of 881-1174 Pa, in the contralateral joints there is also an increase in pressure, but to a lesser extent from 1371 to 1742 Pa. Phlebography is performed under general anesthesia, a contrast agent is injected into the subtrochanteric space, radiographs are performed 5, 10, 20 seconds after its introduction. On phlebograms in the anteroposterior projection, the following vascular formations can be seen:
Superior reticular veins, coming from the upper outer quadrant of the head and upper part of the femoral neck and emptying into the superior gluteal vein.
Inferior reticular veins, originating from the infero-outer quadrant of the head and lower part of the femoral neck and emptying into the femoral vein of the femoral head, running from the internal quadrants of the femoral head to the obturator vein.
Thus, in aseptic necrosis, the pathologically developed type of blood circulation in the hip joint leads to the discharge of incoming arterial blood into the diaphyseal venous system of the thigh, and the tissues of the femoral head are in a state of chronic ischemia.
One of the methods for assessing the blood supply to the hip joint is gamma scintigraphy with 99m Tc-pyrophosphate, 85 Bg, which is administered intravenously 2 hours before gamma scintigraphy. Then the coefficient of differential accumulation of the radiopharmaceutical is determined by the difference in activity per unit area of the affected and intact hip joint, related to the activity per unit area of the intact joint. Normally, the coefficient of differential accumulation of 99m Tc-pyrophosphate in the bones of the hip joint and symmetrical parts of the bones does not exceed 0.05. In aseptic necrosis of the femoral head, the accumulation of 99m Tc-pyrophosphate depends on the stage of the pathological process:
T-TT stage - characterized by a decrease in the accumulation of the drug, which is associated with a decrease in the blood supply to the femoral head, the cause of which is the occlusion of the supply vessels at the level of the joint capsule and the cartilaginous components of the femoral head.
TTT stage - the blood supply is unstable, the inclusion of the radiopharmaceutical is multidirectional and alternates with periods of reduced (with total damage to the epiphysis) and increased accumulation (with signs of resorption of fragmented areas).
TU stage - stable revascularization, the accumulation of the drug in the bones of the affected joint increases again, the stage is accompanied by a steady restoration of the blood supply to the affected joint.
To study the state of regional blood circulation and functional activity of bone tissue, three-phase dynamic bone scintigraphy is used, using 85 Bg, 99m - diphosphonate, 99m Tc - polyphosphate or 99m Tc - phosphone. The labeled radiopharmaceutical is administered intravenously, the study is carried out in a gamma camera. The following is being assessed:
Arterial inflow (T);
Perfusion states (TT);
Functional activity of bone tissue (TTT).
The analysis of the first two phases includes initially projective identification of areas of interest in the area of the common iliac (the level of the bifurcation of the abdominal aorta) and the external iliac (the level of the bifurcation of the common iliac artery) arteries, in the area of the femoral head, as well as in the projection of the medial and lateral arteries, circumflex thigh on the affected and healthy limb. Further, curves "activity / time" are built taking into account the area, the time of collecting information, the integral values for the curves and the percentage of the difference between the affected and healthy sides are calculated.
In a scintigraphic study of patients with stage T disease, accumulation of the radionuclide in the pathological focus is noted, which is explained by limited aseptic necrosis, destruction of bone tissue and bone marrow hemorrhages. In patients with stage TT disease, accumulation of the radionuclide in the focus of necrosis is observed with increased intensity compared to healthy epiphysis, due to the process of resorption of necrotic tissues, revascularization and the onset of bone proliferation. In the TTT stage, the accumulation of the radionuclide is uniform in intensity and homogeneity both in the diseased and healthy epiphysis, since bone proliferation has ended and new bone formation has begun.
To assess the intensity of blood circulation in the lower extremities, methods of rheography, digital plethysmography, and skin thermometry are used. Registration of records of rheograms and plethysmograms is carried out on a six-channel electrocardiograph and on an eight-channel polygraph. An electrothermometer measures the temperature of the skin in the inguinal regions, on the front surfaces of the thighs and lower legs in the middle third and on the rear of the feet. According to the rheogram, the rheographic index is calculated, according to the plethysmogram, the volumetric pulse on the first toe is determined. In sick children, according to rheography data, there is a tendency to reduce the intensity of blood circulation in the diseased thigh, a significant difference in the volumetric pulse of the 1st toes is determined with a tendency to decrease blood supply to the distal lower extremities on the diseased side, plethysmography indicators are reduced on the diseased side. In the study of patients with Perthes disease, M.N. Kharlamov et al (1994) showed that there is a decrease in thermogenic activity on the affected side. At the stage of synovitis in the area of the affected joint, an increase in the intensity of heat radiation is determined. With an impression fracture, zones with reduced heat radiation appear.
Radiation methods for the study of the hip joint.
The leading methods for diagnosing aseptic necrosis and osteochondropathy of the femoral head are radiation methods. The traditional radiation method is radiography. However, the complex and diverse nature of morphological and functional changes in the affected joint, its vascular bed, and in the entire limb as a whole make the method of traditional radiography insufficiently informative. In recent years, new effective methods of radiation diagnostics have appeared in traumatology and orthopedics. Among them are computed and magnetic resonance imaging, X-ray angiography, sonography and other research methods.
There are five stages of radiographic manifestations of aseptic necrosis:
T stage - X-ray changes are practically absent, this period is called latent. It lasts no more than 10-12 weeks. In this stage, there may be a normal radiological picture or minimal osteoporosis, there is a mild uneven compaction of part or the entire epiphysis, gradually turning into an unchanged structure, due to the presence of necrobiosis and necrosis of bone remodeling in the area with a predominance of endosteal bone formation. A slight expansion of the joint space and a decrease in the height of the epiphysis compared with a healthy limb, which occurs due to a violation of endochondral ossification. V.P. Gratsiansky (1955) believes that some rarefaction of bone tissue is detected in the femoral neck at this stage. A number of changes in the head and neck of the femur were also identified by other authors.
TT stage - radiologically, the femoral head is devoid of a structural pattern, compacted, homogeneous, a thin band of enlightenment is observed around the compacted area of the epiphysis and a further decrease in the height of the epiphysis. These changes are due to perifocal resorption and secondary necrosis, which causes a violation of osteogenesis, which is manifested radiologically by the expansion of the joint space and a partial decrease in the height of the epiphysis.
The TTT stage is radiographically the most indicative in terms of the depth of structural changes that have arisen, resorption of the necrotic area is revealed, characterized by a decrease in its height and fragmentation, the continuous shadow of the head is divided into sequester-like, structureless areas of various configurations, expansion of the growth zone and restructuring of the structure in the adjacent metaphysis is often observed. The epiphyseal cartilage loosens, its relief is uneven, thickened,
the articular cartilage is thickened, radiologically this is manifested by the expansion of the joint space.
TU stage - a clear epiphyseal plate is determined radiographically, the beam structure of the epiphysis is restored, sequester-like bone fragments disappear. Sometimes there are cystic enlightenments with sclerotic rims, the structure in the area of the former necrosis and in the adjacent part of the bone becomes more uniform (restoration of the structure begins from the periphery). The height of the epiphysis increases and the width of the joint space decreases due to the normalization of endosteal and endochondral bone formation. The structural pattern of the head is rough, the direction of the trabeculae is random.
At the stage, when the femoral head is damaged and the process spreads to the growth zone, its premature closure is noted, as a result of which the limb is shortened. Uneven damage to the growth zone leads mainly to the development of varus deformity of the proximal end of the femur. In these cases, secondary degenerative-dystrophic changes occur early in the form of deforming arthrosis, cystic restructuring and repeated necrosis.
The course and outcome of aseptic necrosis of the femoral head depend on the extent and localization of the lesion of the femoral head. O. V. Dolnitsky (1991) distinguishes three forms of damage to the femoral head, which differ from each other in the localization and size of the focus of necrosis caused by the blockade of various areas of the blood supply to the femoral head:
1. The small-focal form is characterized by the minimum size of the lesion. With this form, its subchondral and medial localization is possible: a small, narrow sequester-like shadow is determined under the dome of the head or at the medial edge of the epiphysis. With a small-focal form, the area of bone necrosis covers the area of blood supply to the artery of the round ligament of the thigh - the subchondral variant or the inferior cervical artery (a branch of the medial circumflex artery of the thigh) - the medial variant.
2. Limited form. The anterior central segment of the head is affected. On the roentgenogram in a direct projection, a dense structureless fragment is limited by a band of enlightenment from the outer and inner segments of the epiphysis. The affected area rarely reaches the growth plate, more often a layer of spongy bone remains between them. With this form of damage, the outer segment of the epiphysis is not completely resorbed. In the lateral projection, the area of necrosis covers the anterior part of the ossification nucleus, sometimes spreading in a narrow strip under the articular cartilage to the center
epiphysis. There is a slight expansion of the epimetaphyseal zone. Rarely, cystic formations are found in the anterior sector of the metaphysis, communicating with the germ plateau. With a limited form, the area of bone necrosis covers the area of blood supply to the superior cervical artery (a branch of the medial circumflex artery of the thigh).
3. Common form. The most extensive lesion of the femoral head. In this case, the outer section of the epiphysis always suffers. With a subtotal lesion of the impression and subsequent fragmentation, about 2/3 of the ossification nucleus undergoes. Only the posteromedial region of the epiphysis does not resolve. The total lesion of the ossification nucleus is accompanied by its pronounced impression: it thickens, turning into a narrow strip, then completely fragments and resolves. Fragments of the epiphysis can be introduced into the growth zone, which is significantly defibrillated and unevenly expanded. In areas of the metaphysis adjacent to the growth zone, as a rule, cystic formations are detected. In children older than 8 years, often with this form of lesion, pronounced osteoporosis of the femoral neck is observed up to its complete osteolysis. Less commonly (in children under 6 years of age), the metaphysis remains intact. The common form corresponds to the defeat of all branches of the medial circumflex artery of the thigh: the superior cervical artery in the subtotal variant and both cervical vessels in the total lesion.
Promising modern methods of radiation diagnostics include computed tomography (CT), which allows early recognition of signs of aseptic necrosis of the femoral head. The essence of the method is to obtain a layered image on a tomograph. The images are obtained as a result of mathematical processing of the data of the absorbed X-ray radiation passing by the beam through the tissues of the patient's body of various density by means of a computer. The density of tissues is compared with the density of water (zero mark) and the density of air (minus 500 units). Bone density can be expressed in plus values. Bone densitometry is based on this principle.
Traditional X-ray examination in the early stages of aseptic necrosis of the femoral head does not reveal pathological changes, the spherical surface of the femoral head is preserved, the joint space remains of normal width. X-ray examination does not always allow answering the question about the exact location and size of the pathological process, the state of the cartilage and paraarticular tissues. Ordinary radiographs do not allow assessing the dynamics of restoration of the bone destruction zone due to a change in the position of the femoral head after corrective osteotomy.
CT can detect the early stage of avascular necrosis of the femoral head. The tomograms show a decrease in the density of bone structures on the affected limb compared to the healthy one. CT allows layer-by-layer, polypositional examination of the structure of the femoral head and neck, to make a qualitative and quantitative assessment of the state of the femoral head and acetabulum with the determination of the general relationship of articular surfaces, the size of cystic cavities and their relationship with areas of bone sclerosis, the state of subchondral bone tissue. The total density of the femoral head is measured at various levels and histograms are plotted taking into account the densitometric characteristics of a healthy hip joint.
CT provides invaluable assistance in the topical diagnosis of the affected area. Axial CT allows you to determine the exact location and size of the area of necrosis of the femoral head, calculate the necessary correction parameters with an accurate recommendation in degrees of angular and rotational displacement of the femoral head in order to remove its necrotic area from under load. As a prognostic indicator of the effectiveness of organ-preserving operations on the hip joint in aseptic necrosis of the femoral head, the ratio of the areas of cystic cavities and areas of sclerosis is used, which can be determined by layered CT. The predominance of areas of sclerosis over cystic cavities is a favorable prognostic sign. Quantitative densitometry with the construction of histograms of the upper third of the femoral head makes it possible to distinguish 2 types of curves: with unimodal and bimodal density distributions. A healthy femoral head is characterized by a unimodal curve, while with aseptic necrosis of the femoral head, either a bimodal curve or a unimodal curve is observed with a density peak shift to a denser side. CT studies allow assessing the degree of compaction of para-articular tissues and the presence of intra-articular fluid. According to these signs, along with laboratory studies, one can judge the activity of a nonspecific inflammatory process in the hip joint.
At the final stage of the study, a picture of the topographic section of the object under study is issued. The image is based on objective information about the degree of X-ray density of various parts of organs and tissues. The obtained tomograms allow assessing the state of bone structures, the degree of anatomical disorders.
Unfortunately, CT equipment is quite expensive and not all clinics, even regional ones, are currently equipped with it. Given the fact that CT
requires prolonged immobility of the patient; for young children, this study is possible only under conditions of drug sleep. Nuclear magnetic resonance imaging (NMRI) has unique capabilities in the diagnosis of the initial (pre-radiological) stages of aseptic necrosis of the femoral head, which makes it possible to obtain more complete information about the state of the femoral head and surrounding tissues, taking into account the cartilaginous and soft tissue components. Unlike the X-ray method, with NMRI, a safe interaction occurs between radio waves and certain cell nuclei under the influence of a magnetic field. Under the influence of a magnetic field, the hydrogen proton, which is part of the tissues of the body, changes its orientation, which is recorded on the monitor screen by a glow of various intensities. The more water in the tissues, the brighter the glow of this zone on the cut, the areas of the cortical bone in the image look dark. When analyzing NMRI data, it should be taken into account that a strong signal gives a white color, the weakest signal is black, which depends on the fluid content in the tissues. NMRI is performed in T1 and T2 modes, 4-5 slices 5 mm thick are performed, with an interval of 1-2 mm. In aseptic necrosis, the affected bone marrow of the femoral head produces little or no signal.
In the first stage of aseptic necrosis on a series of coronary and transversal tomograms of the hip joints, the femoral head is round and relatively large. In the projection of the epiphyses of the femur, areas of hypointensity with clear uneven contours are determined on the edge of the physeal cartilage. The asymmetry of the position of the proximal femur is determined in the form of an increase in anteversion on the side of the lesion, as well as atrophy of muscles and subcutaneous fat, without areas of pathological intensity. Changes in the capsule of the hip joint are manifested in the form of an increase in the strength and volume of the light signal.
In the stage of decompressed ischemia (osteonecrosis, impression fracture, fragmentation) on tomograms, on the side of the lesion, the femoral head is enlarged, deformed, the epiphysis is flattened with changes in its signal characteristics. Areas of hypointensity are noted in T1 mode. A moderate amount of effusion is determined along the posterior contour of the head. From the side of the paraarticular soft tissues, signs of moderate hypotrophy are determined.
In the recovery stage, against the background of the restored bone marrow of the femoral head, there are foci of bone destruction of varying severity on tomograms. Height of the reconstructed bone marrow in the femoral head
the side of the lesion is smaller than on the healthy one, which also corresponds to the x-ray picture. The femoral head on the side of the lesion is deformed: enlarged and flattened. A small amount of effusion is determined along the posterior edge of the head. The cervical-diaphyseal angle decreases or increases. From the side of the paraarticular soft tissues, signs of moderate hypotrophy are determined. The introduction of MRI of the hip joints into practice makes it possible to visually determine the state of the soft tissue and cartilage elements, the synovial environment of the hip joint and their changes during the treatment process. The method is harmless, non-invasive, but quite expensive. The patient is placed in a geometrically constrained space, which is contraindicated for patients suffering from claustrophobia. Studies should not be carried out in patients with cardiac arrhythmias, the time spent on one MRI study is high. In addition, the number of magnetic resonance tomographs in our country is small, research is carried out only in a small number of large medical diagnostic and scientific institutions. The method, like CT, requires prolonged immobility of the patient, so young children have to undergo MRI under general anesthesia. This limits its application.
To identify the initial, pre-radiological stage of the disease, the method of x-ray densitometry is used. This method is objectively characterized by a uniform decrease in the level of bone mineral density in all areas of the proximal femur relative to the age norm by an average of 17%. However, with transient synovitis, there is a decrease in bone mineral density by an average of 2-4%. In patients with a unilateral process 1-3 years ago, osteoporosis of the bones of the affected joint develops with a drop in mineralization, on average, to 68.4% of the optical density of the healthy side, with fluctuations from 45 to 90%.
The study of soft tissue and cartilaginous elements of the hip joint became possible thanks to the introduction of such a method as ultrasound sonography. Ultrasound examination of the hip joints allows diagnosing with a high degree of certainty the manifestations of ischemic necrosis of the femoral head with a qualitative characteristic of its severity. The method is highly informative, non-invasive, fast in real-time execution, with the possibility of multiple execution and evaluation of the process dynamics, and relatively cheap. Today, ultrasound is undoubtedly the method of choice in diagnosing changes in various organs, including changes in the hip
joints. The value of this method lies in the fact that it can be used repeatedly without risk to the health of patients, in contrast to radiography, which in children, especially newborns, should be used only when necessary.
The method of ultrasonography is based on the location of various organs and tissues by ultrasonic vibrations located in the diagnostic frequency range from 2 to 15 MHz. The small wavelengths of these oscillations are comparable to the distance between the small structural elements of the studied tissues, and the energy release during reflection is minimal, which eliminates the damaging effects of ultrasound.
To understand the biological effects of ultrasonic radiation, it is necessary to know its physico-chemical primary effect. First, the effect of heat generation. The tissue heating temperature depends on the duration of irradiation, radiation intensity, absorption coefficient and tissue conductivity, on the one hand, and on the other
From the amount of heat transfer. The therapeutic use of high intensity ultrasound has been carried out with the use of ultrasonic irradiation devices for a long time. With the diagnostic parameters of ultrasound, heat generation does not play any role.
Secondly, the phenomenon of cavitation, which occurs only with therapeutic, and not with diagnostic intensity of ultrasound radiation. Therapeutic ultrasonic radiation leads to the formation of gas bubbles in the liquid and tissues. When they subside during the pressure phase, high pressure and temperature readings occur, which can secondarily lead to rupture of cells and tissues. Oscillations of oscillating bubbles usually occur asymmetrically, and the emerging movements of the liquid and plasma form a kind of flow. The resulting frictional forces could theoretically cause damage to cell membranes.
Thirdly, the chemical action of ultrasound. Yaoi (1984) described the effect of depolymerization of macromolecules. This effect has also been proven in experiments on various protein molecules and isolated DNA. The occurrence of this effect in cellular DNA is impossible due to the too small size of the molecules, therefore, the mechanical energy of the wavelength cannot affect the formation of depolymerization.
All primary effects of ultrasonic radiation depend on the intensity of the ultrasonic wave and its frequency. The power of currently used devices in the range of 5-50 mW/cm2 lies significantly below the threshold of the experimentally created possibility of damaging action. Diagnostic use
ultrasound, thus significantly different from ionizing radiation, in which the primary effect does not depend on dose and intensity.
Ultrasound has been used for diagnostic purposes for almost 30 years and no damaging effect of this diagnostic method has been proven to date. Given the current level of scientific research, it can be argued that the ultrasound method with the intensity used is safe and does not pose any risk to the health of the study population.
With the advent of new ultrasonic scanning methods, scientific research is constantly being conducted to study the effect of the technologies being introduced on biological tissues. The European Committee for the Safety of Ultrasound in Medicine (ECMUS) of the European Federation of Societies for the Application of Ultrasound in Medicine and Biology (EFSUMB) has developed recommendations for new technologies that affect biological tissues. The Clinical Safety Instructions (1998) recommends that the user use the information provided by the manufacturer when performing Doppler ultrasound. There are safety indexes - thermal (TI) and mechanical (MI) for exposure control. The first of them takes into account possible thermal effects, the second - cavitation effects. If there are no indexes on the screen of the device, the doctor should reduce the exposure time as much as possible. In orthopedic studies, TI should not be higher than 1.0, MI should not be higher than 0.23 at the intensity of the ultrasonic pulse Ispta (maximum in space, average in time intensity) not more than 50 mW/cm2. Ultrasound diagnostic devices currently on the market operate at intensities that are well below those set by the American Institute for Ultrasound in Medicine based on the in vivo AIUM (American Institute for Ultrasound in Medicine) Statement.
An ultrasonic wave reflected from small elements of tissue structures and at the boundaries of media between different tissues is captured by the device. After multiple amplification and complex transformations, a two-dimensional image is built on the monitor screen in the so-called "gray scale". Modern devices allow not only to obtain a static image, but also to conduct research in real time. Not all tissues of the body have good imaging characteristics, which limits the application of the technique. Another disadvantage of ultrasonography is the subjectivity of assessments, which depends on the characteristics of the image and the practical experience of the researcher. Despite these
Limitations The diagnostic advantages of ultrasonography are indisputable; it has found its application in all branches of medicine, including orthopedics.
Visualization of biological structures using ultrasound technology is carried out in two-dimensional mode (B-mode) using the Doppler effect (duplex scanning), which allows you to study the anatomical structure of organs and study the blood flow in them. Ultrasound examination of the structures of the hip joint allows visualizing the contours of the edge of the acetabulum, the head and neck of the femur, the articular capsule adjacent to the head and neck of the femur, the growth zone between the epiphysis and metaphysis of the femoral head, the cartilaginous cover of the femoral head.
Ultrasonic methods for studying the hemodynamics of the hip joint.
The Doppler effect, described by the Austrian physicist H.A. Doppler, lies in the fact that the frequency of the ultrasonic signal, when it is reflected from a moving object, changes in proportion to the speed of the located object along the signal propagation axis. When the object moves towards the radiation source, the frequency of the echo reflected from the object increases, and when the object moves away from the radiation source, it decreases. The difference between the transmitting and receiving frequencies is called the Doppler frequency shift. The magnitude of the ultrasound frequency shift can determine the speed and direction of blood flow [V.P. Kulikov, 1997].
In 1980 P.G. Clifford et al. used a duplex method for examining blood vessels. The advantage of duplex scanning is the possibility of simultaneous echolocation of the vessel in real time and analysis of Doppler spectrograms of blood flow. In addition, the method makes it possible to calculate the real values of the linear and volumetric blood flow velocity by correcting the angle of inclination of the sensor to the longitudinal axis of the vessel. The combination of B-mode vessel imaging, color flow mapping and spectral analysis of blood flow is referred to as triplex scanning. Color Doppler mapping (CDC) is a mode that allows you to trace the spread of the blood flow, the marginal filling defect corresponds to the parietal formation, and the color flow corresponds to the true diameter of the vessel. When an artery is occluded, a break in the color cartogram is determined. Doppler spectrography is the most sensitive method for assessing the nature of blood flow in different parts of the vessels. A new mode of ultrasound diagnostics - power Doppler mapping, is based on the analysis of the amplitude of ultrasonic vibrations reflected from
moving objects, the information is presented on the display in the form of color-coded blood flows. Unlike color doppler imaging, power Doppler mapping (EDC) is not sensitive to the direction of flow, is little dependent on the angle between the ultrasound beam and blood flow, is more sensitive especially to slow flows (it is possible to study low-velocity arterial and venous blood flows), and is more noise-resistant.
Doppler ultrasound has found wide application in orthopedics. In the practice of orthopedics - traumatology, it often becomes necessary to study blood flow in the limbs, especially in areas of interest. Previously used angiography has not found wide distribution, as it is an invasive method and is intended mainly for a single study. At present, in connection with the development of ultrasound diagnostic equipment, it became possible to monitor regional hemodynamics in patients with pathological processes of inflammatory and degenerative-dystrophic origin. Modern ultrasound devices, with the ability to conduct color Doppler mapping, provide the highest resolution of diagnostic images of ligaments, tendons, cartilage. At the same time, it is possible to assess the vascular response in the area of the detected changes, as well as to monitor the treatment.
Using the method of color flow, changes in blood circulation in the hip joint area were found, which occur during its congenital and acquired pathology, as well as in the course of ongoing medical manipulations. In this case, the blood flow can be traced both in the soft tissues surrounding the hip joint and in the structures represented by cartilaginous tissue. In the process of research, some regularities are determined:
Decreased blood flow in the hip joint area in children with Perthes disease, congenital unilateral hip dislocation, and with deforming arthrosis, in comparison with the conditionally healthy side, which once again proves the pathogenetic nature of these diseases and makes it possible to conduct appropriate therapy with control of blood circulation in the area of interest.
After surgical interventions, using various implants, ultrasound studies with color Doppler mapping make it possible to visualize the processes of transplant restructuring. At the same time, an increase in blood flow in the implant area and a decrease in the level of peripheral resistance in the vessels (IR - 0.4-0.7) are indirect signs of the ongoing restructuring, and a subsequent decrease in the number of arterial vessels and an increase in
peripheral resistance (IR approaches 1.0) in them indicates the completion of the process.
In inflammatory processes in the area of the hip joint, CDI detects an increase in blood flow in the area of the joint capsule, synovial membrane. According to the degree of vascularization, one can conditionally speak about the severity of the process, and later, during the treatment process, monitor the ongoing changes.
In order to visualize microcirculation in the area of the hip joint in children of early and younger age with congenital hip dislocation, the method of power Doppler mapping was used. The method is based on the amplitude of the echo signal, which reflects the density of moving erythrocytes in a given volume, without taking into account the speed and direction of movement. Therefore, with the help of EHD, it is possible to obtain images of vascular structures not only with a high flow rate in them, but also small vessels with a very low blood flow rate. In this regard, EDC in most cases is used to visualize the microvasculature of the vascular bed. When performing energy mapping of the hip joint area, Doppler signals are recorded in the projection of the cartilaginous part of the roof of the acetabulum, limbus, in the centers of ossification of the femoral head, in the proximal growth zone of the femur, joint capsule and muscle tissue. In patients with unilateral congenital hip dislocation, it was noted that the power of Doppler signals is always 2.1 times lower on the side of the lesion. With dysplasia with a delay in the development of the nucleus of ossification of the femoral head, there is a decrease or absence of the Doppler signal in the center of the femoral head, which indicates a decrease in blood flow in this area.
Duplex ultrasound examination of venous blood flow in children with osteochondropathy of the femoral head reveals secondary changes in the diameter of the venous vessel against the background of the existing venous pathology. Venous dilatation leads to severe hemodynamic disorders of the proximal femur resulting from acute thrombosis, accompanied by gross trophic disorders of the bone tissue in cases of late diagnosis and untimely treatment. The technique of duplex scanning of the lower extremities in children revealed a pattern of a significant increase in venous stasis (50% or more) on the affected side in Legg-Calve-Perthes disease in combination with a certain ultrasonographic characteristic of the bone and cartilage components. These data facilitate the identification of the pre-radiological stage of the disease - the stage of latent ischemia,
which can be a highly informative method for early and differential diagnosis of diseases of the proximal femur.
Thus, Doppler ultrasound, which allows to assess the regional blood supply of the hip joint in aseptic necrosis of the femoral head, synovitis, arthritis, is an important method for assessing the effectiveness and adequacy of the treatment, load regulation and functional therapy.
Ultrasonic research methods for a number of pathologies of the hip joint.
Pain in the hip joint in children can occur for various reasons: with Legg-Calve-Perthes disease, transient synovitis, coxarthrosis and other diseases of the hip joint. The problem of early diagnosis of aseptic necrosis of the femoral head is the most relevant in pediatric orthopedics. Late diagnosis of degenerative disorders in the femoral head leads to a large percentage of poor outcomes with subsequent development of coxarthrosis. Ultrasonographic signs of aseptic necrosis of the femoral head have been described by a number of authors.
At the stage of necrosis, signs of synovitis are determined: expansion of the joint space due to effusion in the joint, decrease in the acoustic density of the head sections, foci of loosening of the epiphysis, heterogeneity of the acoustic density of the head sections, heterogeneity of the acoustic density of the growth zone, moderate "blurring" of the contours, a violation of the shape of the cartilaginous part of the head. Joint effusion on ultrasonography, as the first manifestation of the pre-radiological stage, occurs in 50% of cases.
At the stage of an impression fracture, a moderate accumulation of effusion in the joint cavity, a decrease in the height of the epiphysis, and multiple areas of increased acoustic density are detected. Flattening, fuzziness and discontinuity of the contours of the head may also be noted.
At the fragmentation stage, the expansion of the joint space is visualized, a further decrease in the height of the epiphysis, flattening and fragmentation of it, a total decrease in the acoustic density of the ossified part of the head, and the appearance of areas of heterogeneity are determined. Discontinuity and expansion of the head, clumping of its contours are noted.
The reparation stage is characterized by a change in the shape of the head, its flattening of varying severity, an increase in acoustic density, and a change in anatomical relationships in the joint.
The stage of the outcome depends on the previously started treatment, it can be favorable with a complete restoration of the height of the epiphysis of the femoral head and unfavorable when sclerosis is noted, the presence of osteophytes, free intraarticular bodies, the shape of the head is sharply disturbed.
It is well known that successful treatment of aseptic necrosis of the femoral head is possible only in cases where the femoral head has sufficient plasticity and growth potential for its own remodeling. It depends on the stage and severity of the pathological process, the age of the child. The acetabulum in the early stages of the disease retains its correct shape and acts as a matrix for the recovering femoral head. Covering the head completely, the arch of the acetabulum prevents its growth in the lateral direction, thereby preventing further deformation. Otherwise, the typical outcome of the disease is the deformation of the proximal end of the femur in the form of a mushroom-shaped head, which is much larger than the acetabulum, shortening and expansion of the neck and high standing of the greater trochanter. The mushroom-shaped enlarged femoral head destroys the arch of the cavity, which leads to joint instability, which, together with the shortening of 1.5-2 cm, is the cause of lameness.
The described severe violations of the anatomical structure of the hip joint underlie the development of deforming coxarthrosis, accompanied by stiffness, severe pain syndrome and leading to early disability of the patient. Go to the table of contents >>>
Bibliography.
1. Abakarov A. A. Stimulation of reparative osteogenesis in aseptic necrosis of the femoral head in experiment / A. A. Abakarov, A. B. Bogosyan, A. V.
Melgunov // Orthopedics traumatology and prosthetics.- 1986.- No. 11.- P. 14-17.
2. Abalmasova E. A. Osteochondropathy /E. A. Abalmasova // Orthopedics and traumatology of childhood.- 1983.- Ch. 14.- S. 285-293.
3. Antipova A. A. Aseptic necrosis of the epiphyses of bones during the growth period / A. A. Antipova, E. A. Rulla, N. F. Moroz // Proceedings of the VIII Congress of Traumatologists and Orthopedists of the Ukrainian SSR: Sat. scientific Art. - Kyiv, 1979.- S. 53-56.
4. Beletsky A. V. Corrective osteotomy of the femur in the treatment of Perthes disease in children / A. V. Beletsky //Clinic and experiment in traumatology and orthopedics: abstracts of reports. jubilee scientific Conference of the Research Center "WTO", January 26-28. - Kazan, 1994. - S. 14-15.
5. Belokrylov N. M. An integrated approach to the treatment of osteochondropathy of the femoral head in children / N. M. Belokrylov // Proceedings of the Congress of Traumatologists - Orthopedists of Russia with international participation "New implants and technologies in traumatology and orthopedics": Sat. scientific Art. - Yaroslavl, 1999.- S. 502-503.
6. Belyaeva A. A. Angiography in the clinic of traumatology and orthopedics / A. A. Belyaeva.- M.: Medicine, 1993.
7. Bergaliev A. N. Three-phase dynamic bone scintigraphy in complex diagnostics and evaluation of the effectiveness of conservative treatment of neurodysplastic lesions of the hip joint in children /A. N. Bergaliev, A. I. Krasnov // Proceedings of the Congress of Traumatologists - Orthopedists of Russia with international participation "New implants and technologies in traumatology and orthopedics": Sat. scientific Art. - Yaroslavl, 1999.
8. Bunin E. A. Long-term results of surgical treatment of Perthes disease in children in a sanatorium / E. A. Bunin // Orthopedics traumatology and prosthetics.-
1990.- No. 2.- S. 20-23.
9. Varshavsky I. M. Osteochondropathy of the foot and lower leg: textbook - method manual / I. M. Varshavsky. - Samara, 2001.
10. Vasiliev A. Yu. The value of X-ray computed tomography in the diagnosis of certain diseases of the hip joint. Possibilities of modern radiation diagnostics in medicine /A. Yu. Vasiliev, A. V. Zolotarev. - M., 1995.
11. Vashkevich D. B. Ultrasound diagnosis of Perthes disease in children in the pre-radiological phase / D. B. Vashkevich, M. V. Permyakov // Topical issues in the treatment of diseases and injuries of the musculoskeletal system in children.- St. Petersburg, 1997.-C .166.
12. Veselovsky Yu. A. Dystrophic diseases of the hip joint in children: pathogenesis, clinic, treatment / Yu. A. Veselovsky: dis. ... Dr. med. nauk.- L., 1990.- 307p.
13. Veselovsky Yu.A. Pathogenesis and early conservative complex treatment of the initial stages of osteochondropathy of the femoral head in children / Yu. A.
Veselovsky // Orthopedics traumatology.- 1988.-№ 6.- P. 51-52.
14. Veselovsky Yu. A. Surgical treatment of Perthes disease at the beginning of the formation of external subluxation of the femoral head. Early detection, clinical examination and treatment of children with diseases of the musculoskeletal system / Yu. A. Veselovsky.- L., 1991.
15. Vlasov V. V. Introduction to evidence-based medicine / V. V. Vlasov.- M.: Media Sfera, 2001.- 392p.
16. Vlakhov N. Bone scintigraphy in Legg-Calve-Perthes disease / N. Vlakhov, P. Tivchev // Medical Radiology. - 1984.- T. 29.- No. 1.-S. 72-74.
17. Volkov M.V. Osteochondropathy of the femoral head in children / M.V. Volkov // Healthcare.- 1959.- No. 6.- P.21-25.
18. Gankin A.V. On the issue of surgical treatment of Perthes disease in older children / A.V. Gankin, G. M. Chochiev, V. K. Gankina // 8th Russian National Congress "Man and his health", November 24-28. 2003 - St. Petersburg, 2003. - S.
19. Gafarov H. Z. Treatment of children and adolescents with orthopedic diseases of the lower extremities / H. Z. Gafarov. - Kazan, 1995.
20. Glantz S. Biomedical statistics / S. Glantz; per. from English. Yu.A. Danilova; ed. N. E. Buzikashvilli, D. V. Samoilova.-M., 1999.- 459p.
21. Goncharova L. D. Biomechanical substantiation of the functional method of treating ostochondropathy of the femoral head in children: dis. . cand. honey. Sciences / L. D. Goncharova.- Kyiv, 1979.- 118p.
22. Goncharova M. N. Morphological characteristics of changes in the femoral head after reduction of congenital hip dislocation / M. N. Goncharova, I. I. Mirzoeva // Orthopedics, traumatology.- 1970.- No. 2.-S. 10-14.
23. Gorbatenko S. A. Ultrasound diagnosis of injuries and diseases of the musculoskeletal system: textbook. allowance / S. A. Gorbatenko.- M .: CIUV, 1991.- 26s.
24. Count R. Sonography of the hip joints of newborns. Diagnostic and therapeutic aspects: guidance / R. Graf; per. with him. V. D. Zavadovskaya. - 5th ed., revised. and extended - Tomsk: Publishing house of Tom. un-ta, 2005.- 196 p.
25. Gratsiansky V.P. Aseptic necrosis of the femoral head in children and adults / V.
P. Gratsiansky.- M.: Medgiz, 1955.- 192 p.
26. Guseynov A. G. Early diagnosis and treatment of Perthes disease with the use of blood supply intensification: author. ... cand. honey. Sciences / A. G. Guseinov.- Rostov, 1994.- 24 p.
27. Guch A. A. Etudes of modern ultrasound diagnostics / A. A. Guch // Study of the abdominal aorta, pelvic vessels and lower extremities. New technologies in ultrasound.- K.: Ukrmed., 2000.- Issue. 1.- S. 192.
28. Daurov A. Sh. Surgical treatment of children with Legg-Calve-Perthes disease: author. dis. ... cand. honey. Sciences / A. Sh. Daurov.- Samara, 1999.- 26 p.
29. Dedushkin V.S. The role of computed tomography in dystrophic diseases of the hip joint / V. S. Dedushkin // Orthopedics traumatology and prosthetics. - 1991. - No. 1. - P. 1-4.
30. Divakov M. G. Aseptic necrosis of bones and rationale for methods of their treatment: author. dis. ... Dr. med. Sciences / M. G. Divakov.- M., 1991.- 36p.
31. Divakov M. G. Early ultrasound diagnosis of osteochondropathy of the femoral head / M. G. Divakov, K. B. Boloboshko //News of Radiation Diagnostics.- 1999.- No. 2.- P. 12-13.
32. Dolnitsky O.V. Variants of blood supply to the hip joint in Perthes disease and their relationship with the course of the pathological process /O. V. Dolnitsky, A. A. Radomsky // Orthopedics Traumatology.- 1987.- No. 10.- P. 45-48.
33. Dolnitsky O.V. Gamma scintigraphic assessment of the blood supply of the hip joint in Perthes disease / O.V. Dolnitsky // Orthopedics traumatology and prosthetics. - 1989.- No. 3.- P.49-51.
34. Dolnitsky O.V. Synovial environment of the joint in Perthes disease: echographic study / O.V. Dolnitsky, A.A. Radomsky // Orthopedics traumatology and prosthetics.- 1988.- No. 10.- P.1-6.
35. Dolnitsky O. V. Forms of damage to the femoral head in Perthes disease / O. V. Dolnitsky, A. A. Radomsky // Orthopedics traumatology and prosthetics. -1991.- No. 5.- S. 55-61.
36. Dudinov V. N. On the intensity of blood circulation in the lower extremities in children with Perthes' disease / V. N. Dudinov // Changes in peripheral circulation (macro- and microcirculation) in injuries and diseases of the extremities: collection of Ivanovo, 1976 .- C .70-73.
37. Dudinov VN Early diagnosis and early treatment of osteochondropathy of the femoral head in children: author. dis. ... cand. honey. Sciences / V. N. Dudinov.- Kazan, 1980.-23 p.
38. Evseev V. I. Biomechanical concept of the pathogenesis of degenerative-dystrophic processes in the hip joint. Coxarthrosis (pathogenesis, clinic, treatment) / V. I. Evseev - L .: LNIITO, 1980.
39. Evseev V. I. Significance of measurements of intraosseous blood pressure in the femoral neck for early diagnosis of Perthes disease in children / V. I. Evseev, V. D. Sharpar // Kazan Medical Journal.-1983.- V. 64.- No. 6.- S. 408-410.
40. Ezhov I. Yu. Post-traumatic aseptic necrosis of the femoral head /
I. Yu, Yezhov, Yu. I. Yezhov // Traumatology and Orthopedics of Russia.- 1996.- No. 1.- P. 22-25.
41. Eskin N. A. Complex diagnostics of diseases and injuries of soft tissues and joints of the musculoskeletal system: dis. ... Dr. med. Sciences / N. A. Eskin.-M., 2000.- 325p.
42. Zorya V.I. Symptom of blockade of the hip joint in aseptic necrosis of the femoral head stage III / V.I. Zorya // Orthopedics and Traumatology.- 1987.- No.
43. Zubarev A. V. Diagnostic ultrasound: musculoskeletal system / A. V. Zubarev.- M.: Strom, 2002.- 132 p.
44. Zubarev A. V. Ultrasound diagnostics in traumatology /A. V. Zubarev, V. E. Gazhonova, I. V. Dolgova.- M.: Firma Strom, 2003.- 176 p.
45. Ivanov A. V. Algorithm for early diagnosis of Perthes disease using computed tomography / A. V. Ivanov, A. I. Kuropatkin, O. A. Malakhov // Topical issues of pediatric traumatology and orthopedics: materials of scientific and practical. conf. det. orthopedic trauma Russia, June 5-7, Moscow.- M., 2001.- p. 79.
46. Ivanov A. V. Diagnosis and treatment of osteochondropathy of the bones of the lower extremities: dis. ... cand. honey. Sciences / A. V. Ivanov. - M., 2001.- 123p.
47. Isakov Yu. F. Surgical diseases in children / Yu. F. Isakov .- M .: Medicine,
48. Kadyrov M. K. Ultrasound examination of the hip joint in aseptic necrosis in children / M. K. Kadyrov, Kh. Sh. conferences.- Samarkand, 2001.- S. 85-86.
49. Kadyrov M. K. Nuclear magnetic resonance imaging in the diagnosis of aseptic necrosis of the femoral head, after conservative reduction of the VVB / M. K. Kadyrov // Actual problems of vertebrology and arthrology: abstracts of scientific-practical materials. conf.. - Samarkand, 2001. - S. 83-84.
50. Kapitanaki A. L. Early diagnosis of osteochondropathy of the hip joint /
A. L. Kapitanaki, M. V. Chepikov, Yu. I. Pozovsky // Vestnik khirurgii im. Grekov.-1977.- T. 118.- No. 3.- S. 30-34.
51. Kitaev V. V. An open letter to ultrasound specialists in medicine / V. V. Kitaev, B. I. Zykin // Medical visualization. - 1997. - No. 2. - P. 51-52.
52. Kovalenko Yu. D. Scope and sequence of diagnostic actions in Perthes disease / Yu. D. Kovalenko, VG Kryuchok // New implants and technologies in traumatology and orthopedics: materials of the congress of traumatologists - orthopedists of Russia with international. participation. - Yaroslavl, 1999.- S. 550-551.
53. Kotkova M. A. Some aspects of sonographic diagnosis of the pathology of the hip joint in children / M. A. Kotkova, T. V. Builova, O. V. Komkova // Actual problems of traumatology and orthopedics: scientific materials. Conf.- Ch.1.- N. Novgorod, 2001.- S. 387-388.
54. Krasnoyarov G. A. Surgical treatment of osteochondropathy of the lower extremities in children / G. A. Krasnoyarov, O. A. Malakhov, S. I. Belykh, K L. Likhotay // Organizational, diagnostic and therapeutic problems of emergency conditions: Sat. scientific tr. scientific-practical. Conf.- Omsk, 2002.- T. 2.- S. 339-340.
55. Krisyuk A.P. Degenerative-dystrophic diseases of the hip joint in children and adolescents: classification, diagnosis, treatment / A.P. Krisyuk // Orthopedics traumatology and prosthetics.- 1986.- No. 11.- P. 67-73.
56. Krupatkin AI Neurovascular component of the dystrophic process and the development of osteonecrosis in Perthes disease //A. I. Krupatkin, O. A. Malakhov, A. V. Ivanov // Bulletin of Traumatology and Orthopedics. N. N. Priorova.- 2002.- No. 2.- S. 73-77.
57. Kryuchok V. G. Providing unloading of the hip joint in the treatment of Perthes disease / V. G. Kryuchok, I. E. Shpilevsky // Organization and treatment of children with orthopedic diseases and injuries: Sat. abstracts interregional scientific-pract. conf. - SPb., 1990. - S. 68-69.
58. Kryuchok V. G. Early diagnosis and complex treatment of Perthes disease: dis.
Cand. honey. Sciences. - M., 1999. - 202 p.
59. Kuznechikhin E. P. Results of duplex scanning of the vessels supplying the proximal femur in degenerative-dystrophic diseases of the hip joint / E. P. Kuznechikhin et al. conference children. traumatologists-orthopedists of Russia.- St. Petersburg, 2005.- S. 215-217.
60. Kulivov V.P. Color duplex scanning in the diagnosis of vascular diseases / V.P. Kulikov. - Novosibirsk, 1997.
61. Kutsenok Ya. B. Congenital dysplasia of the hip joint. Congenital subluxation and dislocation of the hip / Ya. B. Kutsenok, E. A. Rulla, V. V. Melnik. - Kyiv: Health,
62. Li A.D. Transosseous compression-distraction osteosynthesis in aseptic necrosis of the femoral head (Legg-Calve-Perthes disease): hands. on transosseous compression-distraction osteosynthesis / A. D. Li, R. S. Bashirov.-Tomsk, 2002.
63. Lipchenko V. Ya. Atlas of human anatomy / V. Ya. Lipchenko, R. P. Samusev. - 3rd ed., revised. and additional .. - M .: Alliance-V, 1998.
64. Lvov S. E. Early differential diagnosis of Perthes disease in children with pain in the hip area / S. E. Lvov // Man and his health: 8th deg. national Congress, November 24-28, 2003 - St. Petersburg, 2003. - P. 182.
65. Mavyev B. O. Blood supply of the hip joint in osteochondropathy in children / B. O. Mavyev //Orthopedics, traumatology.- 1985.- No. 12.- P. 43-44.
66. Mazurin A. V. Propaedeutics of childhood diseases /A. V. Mazurin, I. M. Vorontsov. -2nd ed., revised. and additional .- St. Petersburg: Folio, 2002.- 928s.
67. Malakhov O. A. The use of thermal imaging is new in the diagnosis of osteochondropathy of the bones of the lower limb / O. A. Malakhov, A. I. Kuropatkin, A. I. Ivanov // Topical issues of pediatric traumatology and orthopedics: materials of scientific and practical. conf. det. orthopedic trauma Russia, Staraya Russa, May 25-27, 2000 - SPb., 2000.-p. 171-173.
68. Malakhov O. A. Developmental disorders of the hip joint: clinic,
diagnostics, treatment: monograph / O. A. Malakhov, M. B. Tsykunov, V. D. Sharpar. - Izhevsk: Udmurt State University, 2005.- 308 p.
69. Malakhov O. A. Neurodystrophic syndrome and Perthes disease: possible
ways of solving the problem / O. A. Malakhov, A. I. Kuropatkin, A. V. Ivanov // Topical issues of pediatric traumatology and orthopedics: materials of the meeting of the main pediatric orthopedic traumatologists of Russia, May 29-30, 2002, Svetlogorsk, .-SPb., 2002. - S. 148-150.
70. Malakhov O. A. New possibilities of ultrasound in diagnostics and observation
hip dysplasia in young children: proceedings of the meeting of chapters. det. orthopedic traumatologists, Russia May 29-30, 2002, Svetlogorsk / O. A. Malakhov. St. Petersburg, 2002.
71. Malakhov O. A. New possibilities of ultrasound examination in pathology
of the hip joint in children / O. A. Malakhov, S. E. Kralina // Man and his health: 8th Russia. national congress, November 24-28 - St. Petersburg, 2003. - P.183.
72. Malakhov O. A. Formation of the hip joint in children and adolescents: anatomical and x-ray studies / O.A. Malakhov, A. K. Morozov, E. V. Ogarev //Optimal diagnostic and treatment technologies in pediatric traumatology and orthopedics, errors and complications: Proceedings of the Symposium det. traumatologists-orthopedists of Russia, Volgograd, 17-19 sept. 2003 - St. Petersburg, 2003. - S. 206.
73. Mikhailova N. M. Idiopathic aseptic necrosis of the femoral head in adults / N. M. Mikhailova, M. N. Malova.- M.: Medicine, 1982.- 136 p.
74. Moiseev S. N. Osteochondropathy of the femoral head in children: a differentiated approach in diagnosis and treatment: dis. . cand. honey. Sciences / S. N. Moiseev. - M., 1994.- 189 p.
75. Moroz N. F. On the pathological mechanisms of the occurrence and development of degenerative-dystrophic lesions of the joints / N. F. Moroz // Materials of the IV Congress of traumatologists and orthopedists of the CIS. - Yaroslavl, 1993.
76. Nazarov E. A. Degenerative-dystrophic diseases of the joints of the lower extremities: author. dis. .dr. med. Sciences / E. A. Nazarov.- M., 1992.- 30 p.
77. Nazarov E. A. Clinical and morphological parallels in aseptic necrosis of the femoral head in adults / E. A. Nazarov // Archive of pathology.- 1989.- No. 1.- P. 26-29.
78. Nazarov E. A. Revascularization of avascular spongy bone in experiment / E.
A. Nazarov, V. G. Papkov, A. A. Fokin // Orthopedics, Traumatology.- 1991.- No. 8.-S. 26-30.
79. Neverov V. A. Treatment of fractures of the femoral neck in elderly patients / V. A. Neverov // Bulletin of Surgery. - 1988. - No. 9. - P. 144-146.
80. Ovchinnikov G. I. Medical rehabilitation of patients with aseptic necrosis
81. Osipov L. V. On the safety of ultrasound diagnostic studies / L.
B. Osipov // Medical visualization.- 1997.- No. 3.- P. 22-31.
82. Osipov L.V. Ultrasonic diagnostic devices / L.V. Osipov.- M.,
83. Osteochondropathy in children. Comparative analysis of radiation research methods / L. M. Badamshina et al. // Medical visualization. - 2004. - No. 3. - P. 7481.
84. Pavlova M. N. Vascular and microscopic changes in the tissues of the hip joint in Perthes disease / M. N. Pavlova, A. A. Belyaeva, B. O. Maviev // Archives of pathology. - 1986. - T. 48, issue . 4.- S. 57-62.
85. Plis A. I. Workshop on Applied Statistics in the ZRBB environment: textbook. allowance /A. I. Plis. - M.: Finance and statistics, 2004. - Part 1. - 288s.
86. Pozdnikin Yu. I. Early surgical treatment of children with severe forms of Perthes' disease / Yu. 35.
87. Polyakova A. G. Dynamics of regional blood flow in the process of complex rehabilitation treatment, including EHF-puncture, in children with Legg-Calve-Perthes disease / A. G. Polyakova, D. B. Vashkevich // 8th Russian National Congress "Man and his health", November 24-28. 2003 - St. Petersburg, 2003. - S. 191.
88. Popov IV Features of blood circulation in the hip joints in children with Legg-Calve-Perthes disease: dis. ... cand. honey. Sciences / I. V. Popov. - M., 2001.229s.
89. Prives M. G. Human Anatomy / M. G. Prives, N. K. Lysenkov, V. I. Bushkovich.-SPb., 2005.
90. Weight gain M. G. Blood supply to human long bones / M. G. Weight gain.- L.: Medgiz, 1938.- 260 p.
91. Prokhorov V. P. Studying the degree of mineralization in idiopathic osteonecrosis of the femoral head according to X-ray photodensitometry data / V. P. Prokhorov, M. G. Karimov // Orthopedia traumatology and prosthetics. - 1980.- No. 12.-S. 35-38.
92. Pulatov A. R. Possibilities of densitometric studies in the differential diagnosis of Perthes disease / A. R. Pulatov, Yu. N. Boyarintseva // Rehabilitation of patients with injuries and diseases of the pelvic bones. New technologies in the treatment of injuries and diseases of the musculoskeletal system: Republican materials. scientific-practical. Conf., September 17-18, 2003 - Yekaterinburg, 2003.-p. 91-92.
93. Pykov M. I. Children's ultrasound diagnostics / M. I. Pykov, K. V. Vatolin. M .: Vidar, 2001.
94. Radomsky A. A. Perthes disease: issues of pathogenesis, course, outcomes and treatment: author. dis. ... cand. honey. Sciences / A. A. Radomsky. - Kyiv, 1989.- 21s.
95. Rasulov R. M. Aseptic necrosis of the femoral head: literature review /
R. M. Rasulov // Traumatology and Orthopedics of Russia. - 2003. - No. 1. - P. 66-76.
96. Rasulov R. M. A new solution in the treatment of aseptic necrosis of the femoral head / R. M. Rasulov, N. V. Kornilov // Modern technologies in
Traumatology, Orthopedics: Mistakes and Complications - Prevention, Treatment: Intern. congress; Moscow, 5-7 Oct. - M., 2004.- S. 140-141.
97. Rebrova O. Yu. Statistical analysis of medical data. Application of the BTAIBISL application package / O. Yu. Rebrova. - M.: Media Sphere, 2002. - 312s.
98. Reinberg S. A. X-ray diagnostics of diseases of bones and joints / S. A. Reinberg - M., Medicine, 1964.- T. 1.- 530s.
99. Seliverstov P. V. Radiation diagnosis of Legg-Calve-Perthes disease: author.
Cand. honey. Sciences. - Obninsk, 2000.- 22s.
100. Sergienko V.I. Mathematical statistics in clinical trials / V.I. Sergienko, I.B. Bondareva.- M.: GOETAR-MED, 2001.- 256p.
101. Sinelnikov R. D. Atlas of human anatomy / R. D. Sinelnikov. - M., 1978. - T. 1.- S. 230-233.
102. Sinelnikov R. D. Atlas of human anatomy / R. D. Sinelnikov, Ya. R. Sinelnikov.
103. Stages of development of dysplastic coxarthrosis in children / V. A. Andrianov et al. // Orthopedics, traumatology and prosthetics. - 1987. - No. 4. - P. 19-20.
104. Stamatin S.I. Features of angioarchitectonics of the hip joint in patients with aseptic coxarthrosis and their surgical treatment /S. I. Stamatin, I. V. Kuznetsova, A. L. Manya // IV Congress of Traumatologists and Orthopedists of the BSSR. - Minsk, 1984.- T. 1.-S. 109-110.
105. Stenton G. Biomedical statistics: Per. from English. / G. Stenton.- M.: Practice, 1998.- 459p.
106. Stetsula V.I. On the role of mechanical factors in the mechanism of adaptive restructuring of the bone / V. I. Stetsula, A. T. Brusko, N. F. Moroz // Orthopedics, Traumatology.- 1983.- No. 8.- P. 10-15.
107. Tilyakov B. T. Blood circulation in the hip joint in Perthes disease / B. T. Tilyakov, L. Yu. Shvabe, V. R. Farkhadi // Medical Journal of Uzbekistan. - 1988.- No.
108. Tikhonenkov E.S. Congenital hip dislocation / E.S. Tikhonenkov // Manual of traumatology and orthopedics.- M.: Medicine, 1997.- T. 3.- S. 248-252.
109. Fafenrot V.A. Perthes disease and transient coxalgia in children / V.A. Fafenrot.- L., 1990.- 92p.
110. Feitz O. Visual anatomy / O. Feitz, D. Moffett: per. from English. - M.: GEOTAR-MED, 2002.- S. 102-105.
111. Kharlamov M. N. Perthes disease in schoolchildren: Clinic, diagnosis, treatment: dis. .cand. honey. Sciences / M. N. Kharlamov.- St. Petersburg, 1994.- 203p.
112. Chuchkov V. M. Age morphology of the conduction apparatus of muscular nerves / V. M. Chuchkov: dis. ... Dr. med. Sciences. - M.; Izhevsk, 1990.- 445p.
113. Sharpar V. D. Perthes disease. Vascular endothelium of the hip joint during electron microscopic examination / VD Sharpar, OA Malakhov, VM Chuchkov // Optimal technologies for diagnosis and treatment in pediatric traumatology and orthopedics, errors and complications: materials of the symposium det. traumatologists-orthopedists of Russia; Volgograd, 17-19 Sept. 2003 - St. Petersburg, 2003.- S. 295-297.
114. Sharpar VD The value of assessing regional circulation in the early diagnosis of Perthes disease /V. D. Sharpar // Surgical correction and restorative treatment of injuries and diseases of the musculoskeletal system in children: materials of Vseros. scientific-practical. conf. det. orthopedic traumatologists: Sat. - Kazan, 1996. - S. 242-243.
115. Sharpar VD Comparative evaluation of some methods of early diagnosis and treatment of Perthes disease / VD Sharpar // Orthopedics, traumatology and prosthetics.-1984.- No. 4.- P. 14-18.
116. Shatsillo OI Osteo-cartilaginous autoplasty in the treatment of metatuberculous coxarthrosis and aseptic necrosis of the femoral head: author. dis. . cand. honey. Sciences / O. I. Shatsillo.- St. Petersburg, 1998.- 28p.
117. Shumada I. V. To the question of the mechanisms of therapeutic effect of intertrochanteric osteotomies in aseptic necrosis of the femoral head / I. V. Shumada, G. I. Ovchinnikov, V. V. Novopashennaya // Orthopedics traumatology and prosthetics.- 1990.- No. 2.- S. 35-39.
118. Shumada I. V. Modern concepts on the etiology and pathogenesis of aseptic osteonecrosis of the femoral head: a review of the literature / I. V. Shumada // Orthopedics, traumatology.- 1991.- No. 3.- P. 66-69.
119. Yanakova O. M. The role of ultrasonography in the early diagnosis of osteochondropathy of the femoral head in children /O. M. Yanakova, V. I. Sadofeva // Materials of scientific and practical. conf. det. orthopedic traumatologists of Russia; Staraya Russa, May 25-27, 2000 - St. Petersburg, 2002. - P. 164-167.
120. Yanakova O. M. Ultrasonographic diagnosis of hip dysplasia, congenital hip dislocation in children of the first year of life. . cand. honey. Sciences / O. M. Yanakova.- SPb., 1994.-16 p.
121. Yanakova O.M. Ultrasonography and painful hip joint in children / O.M. Yanakova, A.I. Krasnov, L.G. Schwartz // Actual problems of traumatology and orthopedics: scientific materials. conf. within the framework of the international forum "Man and Trauma". - Nizhny Novgorod, 2001. - Part 1. - S. 358-359.
122. Abderhalden R. Fruherfassung der Huftgelenksdysplasie imNeugeborenenalter / R. Abderhalden, M. Amato // Nestle Wissenschaftlicher Dienst.- Munchen, 1995.- 55 s.
123. Arie E. Femofal head shape in Perthes disease: Is the contralateral hip abdominal / E. Arie, F. Johnson, M. H. Harrison // Clin. Orthop.-1986.- N 209.- P. 77-88.
124. Arlet J. Diagnostie de l'osteonecrose femur capitale au syade I / J. Arlet, P. Ficat // Rev. Chir. Orthop.- 1968.-V. 54, No. 7.- P. 637-656.
125. J. Arlet, J. P. Millet, A. Gedean, Rev. Rheum.- 1975.-V. 42.- P. 391-396.
126. Axhausen G. Ueber anaemische infarct am Knochensystem und ihre Bedeutung fuer die Lehre von den primaren Epiphyseonecrosen / G. Axhausen // Archy. klin. Chir. - 1928.- Bd 151.- S. 72.
127. Barker D. J. P., Hall A. J. The Epidemiology of Perthes disease / D. J. P. Barker, A. J. Hall // Clin. Orthop.- 1986.-V. 209.- P. 89-94.
128. Batory I. Die Aetiologie des Morbus Perthes und sein Besiehung zu der Dysplasia Capitis Femoris / I. Batory // Z. Ortop.-1982.- Bd. 120, No. 6.- S. 833-849.
129. Batory I. Opinions and comparative observations about the etiology of Legg-Calve-Perthes disease / I. Batory // Arch. Orthop. Traum. Surg.- 1982.- V.100, N 3.- P. 151-162.
130. Bruns J. Verbesserte Fruhdiagnostik der Femurkopfosteonecrose / J. Bruns, M. Heller, J. Knop et al. // Chir.Praxis.-1987/88.- Bd. 38.- P. 693-700.
131. Burwell R. G. Editorial comment / R. G. Burwell, M. H. Harrison // Clin. Orthop.-1986.- N 209.- P. 2-4.
132. Calve J. Sur une particuliere forme de pseudo-coxalgie greffee sur deformations caracteristiques de l'extrerite superieure du femur / J. Calve // Rev. Chir., 1910. - V. 42.- P. 54-
133. Catteral A. Natural history, classification and X-ray sings in Legg-Calve-Perthes' disease / A. Catteral // Acta orthop. Belg.- 1980.- V.46, N 4.-P. 346-351.
134. Clanton Th. O. Osteochondritis dissecans. History, pathophysiologic and current treatment concepts. /Th. O. Clanton, J. S. De Lee, Clin. Orthop.- 1982.- N 167.- P. 50-64.
135. Coleman S. Femoral neck fracture: pathogenesis of avascular necrosis nonunion and late degenerative changes / S. Coleman, C. Compere // Clin.orthop.- 1961.- N 20.- P. 247-252.
136. Coleman B.J. Radiographically negative avascular necrosis: detection with MR imaging /
B. J. Coleman, H. Y. Kressel, M. K. Dalinke // Radiology.- 1988.-V. 168, N 1.- P.30-39.
137. Cruess R. L. Osteonecroses of bone: Current concept as to etiology and pathogenesis /
R. L. Cruess // Clin. Ortop. - 1986. - N 208.- P. 30-39.
138 Chung S.M.K. The arterial supply of the developing proximal end of the human femur /
S. M. K. Chung // J. Bone Jt. Surgery.- 1976.- V. 58-A, N 7.- P. 961-970.
139. Doria A. S. Three - Dementional (3D) contrast - enhanced power Doppler imaging in Legg - Calve - Perthes disease / A. S. Doria, R. Guarniero, F. G. Cunha // Pediatr. Radiol.-
2000.- N 12.- V. 30.- P. 871-874.
140. Doria A.S. Contrast - enhanced power Doppler sonography: assessment of revascularization flou in Legg - Calve - Perthes disease / A. S. Doria R. Guarniero, F. G. Cunha, M. Modena // Ultrasound med. Biol.- 2002.- V. 28, N 2.- P. 171-182.
141. Doria A. S. Contrast - enhanced power Doppler imaging: comparison with scintigraphic phases of revascularization of the femoral head in Legg-Calve - Perthes disease / A. S. Doria,
R. Guarniero, F. G. Cunha // Petadydiatr. Orthop. 2002.-V. 22.- N 4.- P. 471-478.
142. EFSUMB Newsletter.- 1996.- Issue 2.-V.2.
143. Ferguson A.B. Synovitis of the hip and Legg-Perthese disease / A.B. Ferguson // Clin. Orthop.- 1954.- N 4.- P. 180-188.
144. Ferguson A.B. Recent advances in understanding Legg-Perthes disease / A.B. Ferguson // Orthop. Survey.- 1978.-V.1, N 4.- P. 307.
145. Ficat P. Arthrose et necrose / P. Ficat // Rev. Chir.- 1974.- V. 60.- P. 123-133.
146. Ficat R.P. Early diagnosis of osteonecrosis by functional bone investigation / R.P. Ficat // Progress in orthopaedics surgery.- 1981.- V. 5.- P. 17-27.
147. Frasez P. Further experience with discriminant functions in differential diagnosis of hypercalcaemia / P. Frasez, M. Healy, L. Watson // Postgrad. Med.- 1976.- V. 52.- P. 254-257.
148. Genes B. M. Early osteonecrosis of the femoral head: detection in high-risk patients wish MR imaging / B. M. Genes, M. R. Wilson, R. W. Houk // Radiology.- 1988.-V. 168, N 2.-P. 521-524.
149. Gill T.J. Intraoperative assessment of femoral head vascularity after femoral neck fracture / T. J. Gill, J. B. Sledge, A. Ekkernkamp // J. Orthop. Trauma. - 1998.-V. 12., N 7.- P. 474-478.
150. Graf R. The diagnosis of congenital hip joint dislocation by the ultrasonic compound treatment / R. Graf // Arch. Orthop. Trauma Surg.- 1980.- V. 97.- P. 117-133.
151. Graf R. Fundamentals of sonographic diagnosis of infant dysplasia / R. Graf // Pediatr. Orthop. - 1984.- N 4.- P. 735-740.
152. Green N. E. Intraosseous venous pressure in Legg-Calve-Perthes disease / N. E. Green, P. P. Griffin // J. Bone Jt. Surgery.- 1982.-V. 64-A, N 5.- P. 666-671.
153. Harland U. Ultraschallfibel Orthopadie Traumatologie Rheumatologie / U. Harland, H. Salter // Springer-Verlag Berlin etc.- P. 184.
154. Harrison M. H. M. A preliminary account of the management of the painful hip originating from Perthes disease // Clin.orthop.- 1986.- N. 209.- P. 57-64.
155. Harrison M. H. M. Perthes disease treatment with the Birmingham splint / M. N. M. Harrison, Turner M. H., Smith D. N. // J. Bone Jt. Surg.- 1982.- V. 64-B, N 1.- P. 3-11.
156. Hasegawa G. Scintimetry in transient synovitis of the hip in the child / G. Hasegawa, H. Windstrand, T. Gustavson // Acta Oprthop. Scand.- 1988.- V. 59, N 5.- P. 520-525.
157. Hesse B. Does it always have to be Perthes disease? What is epiphyseal dysplasia? / B. Hesse, G. Kohler // Clin. Orthop.- 2003.- Vol. 414.- P. 219-227.
158. Higer H. P. Transistoriche Osteoporose oder Femurkopfnecrose? Fruhdiagnose mit der MRT / H. P. Higer, J. Grimm, P. Pedrosa // Fortsch. Rontgenstr.- 1989.- Bd. 150, H. 4.- S. 407412.
159. Hulth A. Necrosis of the head of the femur / A. Hulth // Acta Chir. Scand.- 1961.-V.
122, N 1.- P. 75-84.
160. Ingman A. M. A comparison between innominate osteotomy and hip spica in the treatment of the Legg- Calve- Perthes disease / A. M. Ingman, D. C. Peterson, A. D. Sutherland // Clin. Orthop.- 1982.- N. 163.- P. 141-147.
161. Jacobs B. Epidemiology of traumatic and nontraumatic osteonecrosis / B. Jacobs // Clin. Orthop.- 1978.- N. 130.- P. 51-68.
of age at disease onset / B. Joseph, G. Varghese, K. Mulpuri // Pediatr. Orthop.- 2003.-V. 23.-
N 5.- P. 590-600.
163. Kayser R. Value of ultrasound diagnosis in Legg - Calve - Perthes disease / R. Kaiser, J. Franke, K. Mahlfeld // Scweiz. Rudsch. Med. Prax. - 2003.-V. 99, No. 24.- P. 1123-1127.
164. Klisic P. J. Perthes disease / P. J. Klisic // Int. Orthop.- 1984.-V. 8.- P. 95-102.
165. Landin L. A. Transient synovitis of the hip. Its incidence, epidemiology and relation to Perthes disease / L. A. Landin, L. C. Danielsson, C. Wattagard //J. Bone Jt. Surgery.- 1987.- V. 69-B, N 2.- P.238-242.
166. Lausten G. S. Blood perfusion uneven in femoral head osteonecrosis / G. S. Lausten, C.
C. Arnoldi // Acta Orthop. Scand.- 1993.-V.64, N 5.- P. 531-533.
167. Lecuire F. Evolution a long-term de la hanche (Legg-Calve-Perthes) / F. Lecuire, J. Rebouillat // Rev. Chir. Orthop.- 1987.- V. 73.- P. 561-569.
168. Legg A. T. An obscure affection of the hip-joint / A. T. Legg // Boston Med. Surg. J.-1910.- N 162.- P.202-204.
169. Moitrelli G. Osteonecrosis of the hip treated by intertrochanteric osteotomy /
G. Moitrelli, V. Fusco, A. Avai // J. Bone Jt. Surgery.- 1988.- V. 70-B, N 5.- P. 761-766.
170. Nochimson Georgy Legg - Calve - Perthes Disease. (Medline)
171. Orhoseek Meesege Forum. Legg - Calve - Perthes Disease. (Medline)
172. Orler R. Avascular femur head necrosis as severe complication after femoral intramedullary nailing in children and adolescents / R. Orler, O. Hershe, D. L. Helfet // Unfallchirurg.- 1998.- Bd. 101, H. 6.- S. 495-499.
173. Perthes G. Uber Arthritis deformans juvenilis / G. Perthes // Dtsch. Z. Chir.- 1910.- V. 107., N 1-3.- S. 111-159.
174. Portigliatty Barbos M. The biology of idiopathic necrosis of the human femoral head studied by tetracycline labeling and microcardiography / M. Barbos Portigliatty, F. Mica Botto, F. Denicolai // Acta Orthop. Belg.- 1985.-V. 51, N 1.- P.18-27.
175. Salter R.B. The prognostic significanse of the subhondrial fracture and a two-group classification of the femoral head involvement / R. B. Salter, G. H. Thomson // J. Bone Jt. Surg.-1984.-V. 66-B, N 4.- P. 479-489.
176. Schulz R. D. The present of ultrasonography in newborn and young infants hips / R. D. Schulz, M. Zieger // Ann. Radiol.- 1986.-V. 29.- N 8.- P.681-685.
177. Simon G. F. Robben Anterior Joint Capsule of the normal Hip and in Children wish Transient Sinovinis: US Stady with Anatomic and Histologic Correlation / Simon G.F. Robben, Maarten H. Lequin, Ad F.M. Diepstrated // Radiology. - 1999.- V. 210.- P. 499-507.
178. Standard for real-time Display of Thermal and Mechanical Acoustic Output Indices on Diagnostic Ultrasound Equipment // Rockville, Maryland, AIUM/NEMA.- 1992.
179. Starclint H. Microvascular obstruction in avascular necrosis / H. Starclint, G.S. Lausten,
C.C. Arnoldi // Acta Orthop. Scand.- 1995.- V. 66, N 1.- P. 9-12.
180. Steib, J. P. Steib, B. Moyses, J. J. Wenger, Rev. Chir. Orthop.- 1987.- V. 73, N. 8.- P. 601-608.
181. Weiland A. J. Vascularized bone autografts. Experience with a case / A. J. Weiland, J. R. Moore, R. K. Daniel // Clin. Orthop.- 1983.- N 174.- P. 87-95.
182. Welfling J. Embolies micro-particularies et necrose de la tete femorale chez l'adulte / J. Welfling // Rev. Rheum.- 1967.- V. 3, N 2.- P. 126-130.
183. Wells P. N. T. Physical and technical aspects of color flow ultrasound / P. N. T. Wells // Diagnostic Vascular Ultrasound Ed. By Labs K. H. L. - Edward Arnold, 1992. - P. 145-153.
184. Wirth T. Ultrasonography in Legg - Calve - Perthes disease / T. Wirth, G. W.
LeQuesne, D. S. Paterson // Pediatr. Radiol. 1993.-V. 23.- N 4.- P. 331-332.
© Bulletin of the RRCRR of the Ministry of Health of Russia
© Russian Scientific Center for Roentgen Radiology of the Ministry of Health of Russia
Table of contents of the subject "Hip joint (articulatio coxae). Posterior region of the thigh.":Collateral circulation in the hip joint. Collaterals of the hip joint. Collateral vessels of the hip joint.
In the area of the hip joint in the muscles surrounding it, there is a wide network of anastomoses, as a result of which the violation of blood flow through the external iliac and femoral arteries can be compensated (Fig. 4.17). Thus, anastomosis between the lumbar artery and the deep circumflex iliac artery can compensate for impaired blood flow in the area from the aortic bifurcation to the distal external iliac artery.
Occlusion in the area between internal iliac artery and femoral artery compensated for by anastomoses between the gluteal arteries and the ascending branches of the lateral and medial arteries that envelop the femur.
Rice. 4.17. Collaterals of the hip joint 1 - aorta abdominalis; 2 - anastomosis between a. lumbalis and a. circumflexa ilium profunda; 3 - anastomosis a. glutea superior with a. circumflexa ilium profunda; 4-a. iliaca communis; 5-a. iliaca interna; 6-a. glutea superior, 7 - a. circumflexa ilium profunda; 8-a. iliaca externa; 9-a. glutea inferior, 10 - a. obturatoria; 11 - anastomosis between a. glutea inferior and a. obturatoria; 12-a. circumflexa femoris medialis; 13-r. ascendens a circumflexae femoris lateralis; 14-a. circumflexa femoris lateralis; 15-a. profunda femoris; 16 - a femoralis.In the development of collateral circulation the obturator artery also takes part, anastomosing with the medial artery, which envelops the femur.
It should be noted the extremely important role in the development collateral blood flow in the proximal femur deep femoral artery, from which the arteries that surround the femur depart.
HIP JOINT [articulatio coxae(PNA, JNA, BNA)] - a multiaxial joint formed by the acetabulum of the pelvic bone and the head of the femur.
EMBRYOLOGY
By the 6th week of embryonic development, the head of the femur is contoured in the embryo, surrounded by the bodies of the ilium, pubis and ischium. On the 7th week between the flattened acetabulum and the head of the femur, the joint space, the ligament of the head and the transverse ligament of the acetabulum are formed; on the 9th week. T.'s cavity with. basically already done.
Vascular lacunae around T.'s bookmark. appear on the 5th week, on the 6th week the central artery of the limb is formed, from the 7th to the 10th week the vessels form the primary vascular network in the capsule.
Nerve trunks penetrate into the anlage of the limb during the 4-6th week. The first nerve plexuses in the capsule are formed by the end of the 5th month, and on the 6th and 7th months, diverse terminal receptors appear.
ANATOMY
T. s. is a kind of spherical joint (Fig. 1). Three types of movements are carried out in it: flexion-extensor, adduction - abduction, rotational (external and internal rotation).
The head of the femur has the shape of an ellipsoid, less often a spheroid or a ball, covered with hyaline cartilage, the thickness of which at the upper pole, which experiences the greatest vertical pressure, reaches 1.5-3.0 mm, and becomes thinner closer to the edges. The cervical-diaphyseal angle is normally 126-130° in adults.
The acetabulum is the junction of 3 bones - the ilium, pubis and ischium. Its diameter is 47-55 mm, the radius of curvature is 23-28 mm, and the surface area is 33-49 mm2. In the anteroinferior region, the edge of the acetabulum is interrupted by a notch (incisura acetabuli).
In a person, when standing upright, the center of gravity is on a line passing in front of the transverse axis of T. s. The pressure of gravity of the trunk and abdominal organs is directed through the upper parts of the acetabulum to the heads of the femur. The pressure of the ground or support when walking, running or jumping is transmitted through the lower limb to the femoral head and acetabulum.
Capsule T. s. extends from the edges of the cartilaginous lip (labium ace-tabulare) of the acetabulum to the intertrochanteric line, including the entire anterior side of the femoral neck into the joint cavity. Behind the capsule goes to the acetabulum, leaving the back of the femoral neck half open.
The ligamentous apparatus is represented by four ligaments that strengthen the joint capsule, and two intra-articular ones. Extra-articular ligaments T. s.; iliofemoral (lig. iliofemorale) starts from the ilium and, diverging fan-shaped, is attached to the intertrochanteric line, ensures the vertical position of the body, together with the muscles prevents the pelvis from tipping back and limits its lateral movements when walking; the pubic-femoral ligament (lig. pubofe-morale) goes from the lower lateral surface of the superior branch of the pubic bone and the anteromedial edge of the acetabulum to the intertrochanteric line of the femur, weaving into the T.'s capsule; sciatic ligament (lig. ischiofemora-1e) strengthens the posterior part of the articular capsule, extending from the edge of the acetabulum along the entire length of the ischium to the intertrochanteric line and the anterior edge of the greater trochanter of the thigh; in the thickness of the articular capsule, the fiber bundles form a circular zone (zona orbicularis) surrounding the medial part of the femoral neck.
The least strong sections of the capsule are between the ischio-femoral and pubic-femoral ligaments (at the level of the notch of the acetabulum) and at the level of the tendon of the iliopsoas muscle going to the lesser trochanter, under which there is an iliopectineal synovial bursa (bursa iliopecti-pea) , in 10% of cases connected to the joint cavity. Inside T. with. located: ligament of the head of the femur (lig. capitis femoris), connecting the head of the femur with the fossa of the acetabulum, and the transverse ligament of the acetabulum (lig. transversum acetabuli), connecting the edges of the notch of the acetabulum.
Innervation is carried out by the femoral, obturator, sciatic, superior and inferior gluteal and genital nerves, the branches of which, together with the articular branches of the nerve plexuses of the periosteum and vascular nerve plexuses, form a wide-looped nerve plexus of the fibrous membrane and the plexus associated with it by connecting branches in the thickness of the synovial membrane (Fig. .2).
The blood supply is carried out by the medial and lateral arteries that go around the femur (aa. circumflexae femoris med. et lat.) and the obturator artery (a. obturatoria), which gives off branches to the head and neck of the femur, as well as to the acetabulum (Fig. 3). Non-permanent branches go from the first perforating (a. perforans), upper and lower gluteal (a. a. gluteae sup. et int.) and internal genital (a. pudenda interna) arteries to the femoral neck and acetabulum. Along the outer edge of the latter, the widely anastomosing arteries of the hip joint form a closed ring.
The posterior branch of the obturator artery (r. posterior a. obturatoriae) supplies the acetabulum, the fat pad, the transverse ligament of the acetabulum and adjacent segments of the cartilaginous lip, the medial and inferomedial sections of the articular capsule and the ligament of the femoral head, through which the vessels penetrate into the upper section of the head . In a fibrous membrane of a capsule of T. page. the vessels form a large-loop network, anastomosing with a denser network of the synovial membrane.
Outflow of blood from T. page. is carried out mainly through the medial and lateral veins surrounding the femur, into the femoral vein and through the branches of the obturator vein into the internal iliac vein.
Lymph, the vessels that go along the blood vessels collect lymph from the deep and two superficial networks of lymph, capillaries located in the synovial membrane and go in front to the external iliac, behind - to the internal iliac lymph nodes.
X-ray anatomy. In the education of T. s. the bones having the wrong form participate, to-rye give difficult projection rentgenol. picture; it can become even more complicated with joint deformities, changes in the position of the patient, including due to careless styling during radiography.

At rentgenol. the study should also take into account the age-related features of the bones that make up the hip joint, associated with structural transformations, to-rye are determined by x-ray examination and are regarded as the age norm (Fig. 4).
In newborns, the cartilaginous head of the femur has a regular spherical or oval shape. The nucleus of ossification in it appears in the first half of the year and grows vigorously towards the ligament of the head, increasing approximately 10 times by the age of 5-6 years. The neck of the femur grows up to 20 years; in the first years of life, its lower and rear sides especially increase. The cervical-diaphyseal angle in children of the first months is on average 140 °.
The acetabulum in newborns is formed by the bodies of the ilium, ischium and pubic bones and the Y-shaped cartilage connecting them. In the first years of life, the bone “roof” of the cavity grows intensively; by the age of 4, a protrusion forms along its outer edge. By the age of 9, there is a partial synostosis of the ilium and pubic bones and a complete synostosis of the pubic and ischial. By the age of 14-15 in girls and by 15-17 years in boys, complete synostosis of all bones occurs in the area of the acetabulum.
For definition on the roentgenogram of ratios of bones in T. page. several landmarks associated with anatomical formations and geometric constructions were proposed (Fig. 5): the “tear figure” formed by the inner wall of the acetabulum and the wall of the pelvic cavity in the region of the notch of the acetabulum, the “crescent figure” formed by the groove between the posterior part of the lunate surface and body of the ischium; a vertical line (Ombredanna) drawn through the outer edge of the arch of the acetabulum; angle a formed by a horizontal line drawn through the symmetrical sections of the Y-shaped cartilage on both sides, and a line passing through the outer and inner points of the arch of the acetabulum; arcuate line (Shenton) drawn along the upper edge of the obturator foramen and extended outward to the inner edge of the femoral neck.
Normally, the “tear figure” has the same shape and size on both sides and is located at an equal distance from the femoral head; the “crescent figure” is projected onto the lower inner quadrant of the femoral head symmetrically on both sides; a vertical line from the outer edge of the arch of the acetabulum passes outside of the femoral head or through its outer section; angle a is the same in both joints and does not exceed 22-26°; Shenton's line should smoothly, without kinks and ledges, pass from the upper edge of the obturator foramen to the inner edge of the femoral neck. Displacement of the femoral head in relation to the listed landmarks indicates its subluxation or dislocation.
EXAMINATION METHODS
When examining a patient with T.'s defeat, s. reveal a violation of posture and changes in the musculoskeletal system as a whole; determine the degree of elongation or shortening of the limb, its position in relation to the pelvic girdle, the volume of active and passive movements in the joint. In the area of the joint, the presence of deformities (ankylosis, contracture), changes in the contours, volume and shape of the joint, its skin temperature, and also patol are determined. skin changes (hyperemia, scars, ulcerations, fistulas).
The strictly horizontal position of the pelvis (in the standing position), the location of the hips perpendicular to it and moderate lumbar lordosis (see) are considered normal. With flexion contracture T. s. and perpendicular to the installation of the thigh, the lumbar lordosis sharply increases due to the inclination of the pelvis anteriorly. This is especially well revealed when examining a patient in the supine position on a flat hard surface. To determine the angle of the contracture, the healthy leg is bent, thus eliminating the lordosis, while the thigh on the diseased side goes into a flexion position. This angle corresponds to the angle of the flexion contracture. In the presence of the bringing or taking away contracture of T. page. it is possible to set the hips parallel to the longitudinal axis of the body only with a lateral tilt of the pelvis.
About deformation within a neck and a head of a femur judge by a number a wedge, signs, first of all by a ratio of absolute and relative length of an extremity. If the absolute length (from the top of the greater trochanter to the patella or ankle) is the same on both sides, and the relative length (from the anterior superior iliac spine to the patella) is shortened on the side of the lesion, the displacement of the femoral head or varus deformity of the neck is suggested. About T.'s defeat with. can be judged by the presence of Trendelenburg's symptom; the patient is asked to stand on a sore leg, bending a healthy one; while the pelvis tilts to the healthy side. Visually, a change in the position (skew) of the pelvis is perceived by a decrease in the anterior superior spine and gluteal fold on the healthy side (Fig. 6). To keep the body in balance, the patient tilts it towards the pathologically altered T. s. Such a deviation of the body when determining the Trendelenburg symptom is referred to as the Duchenne symptom. Often, especially with congenital hip dislocation, they talk about the Duchenne-Trendelenburg symptom.
For detection of deformation in the area of T. page. several reference points are also used. The most commonly used are the following. Roser-Nelaton line connects the anterior superior iliac spine with the most prominent point of the ischial tuberosity. Normally, with the hip bent at an angle of 135 °, the greater trochanter is located on this line. With dislocation of the hip and varus deformity of the neck, the greater trochanter is displaced above it.
Bryant's triangle is made up of the following lines: a vertical line is drawn through the top of the greater trochanter (in the position of the patient on the back - horizontal) and a perpendicular is lowered from the anterior upper spine; the third line leads from the anterior superior spine to the top of the greater trochanter. An isosceles right triangle is formed. When the greater trochanter is displaced, the isosceles triangle of Bryant is violated. The She-maker line is drawn from the top of the greater trochanter to the anterior superior spine. The continuation of the line normally passes through the navel or slightly higher, and when the greater trochanter is displaced, it is below the navel.
Palpation of the area T. s. aims to identify pain points. The most accessible for palpation of the joint are the areas directly below the middle third of the pupart ligament, behind and slightly above the greater trochanter. Soreness in T. s. they are also detected by tapping on the heel of the outstretched leg or on the large trochanter, simultaneous pressure with the hands on both large trochanters, and passive rotational movements in the joint.
At a research of volume of movements in T. page. proceed from the following normal indicators: extension (backward movement) - 10-15°, flexion (forward movement) - 120-130°, abduction - 40-45°, adduction - 25-30°, external rotation - 45° and inward - 40°. Rotational movements are examined with the patient in the supine and prone position.
The big role in statement of the diagnosis is played rentgenol. study.
Before shooting T. s. in the standard anteroposterior projection, if possible, straighten the lumbar lordosis, for which the patient's legs are bent at the knee and hip joints, then the position of the pelvis is aligned so that the anterior superior iliac spines are located symmetrically in one horizontal plane. In this position, the pelvis is fixed, the healthy leg is unbent, while the diseased leg may be bent, and sometimes abducted or adducted. If rotational movements are preserved, then in order to obtain a correct image of the femoral neck, the limb must be rotated inward by 15-20° from the initial position of the foot in the sagittal plane (Fig. 7). The central beam is directed 3-4 cm outward from the middle of the inguinal ligament.
To obtain an image of the bodies of the iliac, ischial and pubic bones that form the acetabulum, as well as to determine the position of the femoral head during dislocations, an additional, semi-lateral (oblique) projection is taken, for which the patient is placed on his back and rotated 50-60 ° towards the joint being examined. The central beam is directed to the joint perpendicular to the film. The correct laying is controlled by probing the anterior and posterior superior iliac spines of the examined side, which should be located in the same horizontal plane.
To obtain a profile image of the head and neck of the femur, laying according to Lauenstein is used, for which the thigh is retracted and maximally rotated outwards (Fig. 8).
PATHOLOGY
To T.'s pathology with. include malformations, injuries, diseases, tumors.
Malformations
The most common are T. dysplasia, congenital coxa vara and plow valga, congenital dislocation and subluxation of the hip.
Dysplasia T. s. consists in the underdevelopment of the acetabulum, a decrease in its depth, and a discrepancy with the size of the femoral head. A wedge, signs are a little expressed; hip abduction and internal rotation are somewhat limited. The diagnosis is based on hl. arr. on data rentgenol. research.
The underdevelopment of the acetabulum is characterized by its small depth, beveled upward and flattened vault; it is usually accompanied by more or less severe developmental disorders of the femur: delayed appearance and growth retardation of the ossification nuclei of the head, valgus form of the femoral neck. With a pronounced violation of the formation of the femur, the ossification point may consist of many unfused fragments even at the age of 7-12 years. Dysplasia T. s. it is usually bilateral. Treatment of a dysplasia of T. page. - see table.
Congenital coxa vara - varus deformity of the femoral neck, with a cut there is a decrease in the cervical-diaphyseal angle (Fig. 9); occurs more often in boys, can be unilateral and bilateral. The patient has lameness, "duck gait", wide standing of the legs (P-position), a positive Trendelenburg-Duchenne symptom, with a unilateral lesion - shortening of the limb, with a bilateral lesion - pronounced lumbar lordosis. The degree of limb shortening depends on the magnitude of the cervical-diaphyseal angle. Unlike congenital hip dislocation, the femoral head cannot be palpated. Sometimes, on palpation, a highly located greater trochanter is mistaken for the head. With congenital coxa vara, the leg is in the position of some adduction and external rotation, the isosceles triangle of Bryant is disturbed, the greater trochanter is above the Roser-Nelaton line, the Shemaker line is displaced. Abduction and internal rotation of the hip are limited. The epiphyseal line of the femoral head from the oblique (normal) takes a vertical position, this creates unfavorable biomechanical conditions in the area of the epiphyseal zone, its instability; functional overload, trauma sometimes lead to slippage of the epiphysis of the femoral head, epiphysiolysis develops. X-ray diagnostics is not difficult: a significant decrease in the neck-diaphyseal angle is visible; research in two projections is obligatory.
In young children, attempts were made to stop the progression of the process with the help of abduction splints, unloading the joint, but no significant effect was observed. The conservative methods of treatment applied in a crust, time at children - see the table. In children over 12 years of age and in adults, surgical treatment is undertaken, which boils down to reconstruction of the proximal femur in order to eliminate the vicious position of its head and neck by various methods of osteotomy (see) - intertrochanteric angular, scarring, subtrochanteric wedge-shaped ( see Fig. 3, 5 to Art. Osteotomy).
Congenital plow valga - deformation, with a swarm of the neck-diaphyseal angle greater than normal; is much less common than congenital coxa vara. It is believed that the development of plow valga is facilitated by a violation of static factors, for example, the absence of a normal limb load with residual effects of poliomyelitis (see), skeletal malformations. Clinically, diagnosing pox valga is difficult. This deformity can be judged by the low location of the greater trochanter, elongation of the limb, and a positive Trendelenburg-Duchenne symptom. The diagnosis is clarified by radiography - see table.
If the deformity does not cause functional disorders, no special treatment is required. In some cases, when the valgus position prevents the centering of the femoral head in the acetabulum, varization (reduction of the cervical-diaphyseal angle) is indicated by intertrochanteric varus osteotomy (see Fig. 3, 4 to Art. Osteotomy).
Congenital dislocation of the hip refers to one of the relatively frequent and severe orthopedic diseases of childhood; it occurs in 0.2-0.5% of newborns (in girls 5-7 times more often). The existing theories of the etiology and pathogenesis of congenital hip dislocation do not fully explain the causes of the onset and development of this pathology. It is assumed that it is based on the defect of the primary bookmark T. s.
Depending on the degree of displacement and the relationship of the femoral head with other elements of T. s. distinguish between dislocation and subluxation. With subluxation, the femoral head does not extend beyond the edge of the acetabulum; when dislocated, it is located outside it. As the femoral head moves upward, the joint capsule stretches; after a few years, a narrowing of the capsule forms below the head, it takes the form of an hourglass, its wall hypertrophies, sometimes reaching a thickness of 1 cm. The acetabulum is flattened and filled with a hypertrophied round ligament and a fatty pad. The head of the femur is gradually deformed, especially when it is subluxated.
In order to diagnose congenital dislocation of the hip, a preventive examination of the child by an orthopedist is carried out in the first 3-4 weeks. life, again - at 3, 6 and 12 months.
For the diagnosis of congenital dislocation of the hip in the first year of life, the following main signs are used: asymmetry of the skin folds on the hips (there are more folds on the side of the dislocation and they are deeper than on a healthy limb), shortening of the limb with unilateral dislocation, limitation of hip abduction, a symptom of slipping of the femoral head (symptom of Marx). An indirect sign of congenital dislocation or subluxation of the hip is its external rotation. Asymmetry of skin folds is not an absolute diagnostic sign of congenital hip dislocation, it becomes important in combination with other signs. Shortening of the limb with unilateral dislocation in young children is determined in the position of the child on the back: the legs are bent at the hip and knee joints, connecting them together, while placing the feet next to the plane of the table, on which the child lies. On the side of the dislocation, a lower location of the knee joint is noted. Restriction of abduction of the hips is detected when examining the child in the position on the back and stomach, bending the legs at the knee and T. s. and breeding them. Symptom of Marx is detected in the supine position; when the leg is abducted, bent at the knee and T. with., the orthopedist feels the slipping of the femoral head into the acetabulum, accompanied by a characteristic click (reduction), and when adducted, it dislocates. For early diagnosis of congenital dislocation, it is important to identify the symptom of the gluteal-femoral fold: in the position of the child on the stomach on the side of the dislocation, its higher location is noted. At the same time, hypotrophy and some lethargy of the gluteal muscles on the side of the dislocation are observed. The definition of the symptom of the pulse is also of known importance: on the side of the dislocation, the pulsation of the femoral artery below the pupart ligament is weakened, due to the absence of a dense base under the artery (the head of the femur in the acetabulum). In children, lameness, Trendelenburg-Duchenne symptom, pronounced lordosis with bilateral dislocation, incorrect location of the greater trochanter (above the Roser-Nelaton line), displacement of the Shemaker line, etc.
The wedge, the diagnosis of a congenital dislocation of a hip (at newborns it has often presumptive character) has to be confirmed rentgenol. a research, at Krom degree of defeat is defined by disturbance of mutual relations of a head of a femur with the reference points described above (see fig. 10 to the item of Dislocations).

The treatment of congenital dislocation and subluxation of the hip is based on the reduction and centering of the femoral head in the acetabulum by conservative or surgical methods. Until relatively recently, the main method of conservative treatment was the Paci-Lorenz method or, as it is more often called, the Lorenz method, which consists in the forced (under anesthesia) reduction of the femoral head into the acetabulum with fixation of T. s. plaster bandage. The method is traumatic, in some cases leads to aseptic necrosis of the epiphysis of the femoral head, and therefore it was abandoned. Treatment begins at an early age, immediately after the detection of dislocation or subluxation of the femur in a newborn. First of all, with the help of medical gymnastics achieve stretching of soft tissues, especially adductor muscles.Then use one of the devices that hold the thigh in the position of abduction and external rotation: Freyka's soft pillow (Fig. 10, a), Pavlik's stirrups, in older children - a bed bandage or Volkov's functional splint (Fig. 10, b), Vilensky's abduction splint, etc. These devices, without restricting movements in the T. s., hold the femoral head in the acetabulum, creating favorable conditions for the formation of the articular cavity and the proximal femur.
If with the help of functional tires the reduction of the dislocation fails, they resort to the traction method, which is carried out with the help of sticky-plaster pulls along the axis of the thigh upwards (Shede's method) with a gradual breeding of the legs. V. Ya. Vilensky conducts such traction for the abduction splint. Efficiency of traction is checked by palpation according to the position of the head of the femur, - if possible, complete abduction of the hips, the same length of the limb. In some cases, when the femoral head has approached the cavity, it is reduced manually. This manipulation, provided that tissue stretching is achieved, is not traumatic. The average traction period is 1.5-2 months, but sometimes it reaches 3 months. and more. Irreducible dislocations are subject to surgical treatment. Surgical intervention is most effective at the age of 1.5-2 years.
Operations for congenital dislocation are divided into several groups: open reduction, reconstructive operations on the ilium and the upper end of the femur without opening the joint, a combination of open reduction in reconstructive operations and palliative operations. In early childhood, with an underdeveloped articular cavity, an open reduction of the femoral head is performed without deepening the cavity, only by removing the fat body from it. Open reduction with a deepening of the acetabulum has a negative side: the articular cartilage of the head, after reduction, contacts the treated bone, which causes its rapid destruction. Italian orthopedist Codivilla (A. Codivilla) in 1900 proposed, and P. Colonna in 1932 developed the technique of capsular arthroplasty. The stretched joint capsule is isolated, thinned by the fibrous layer and, without tension, the head of the femur is wrapped around it in the form of a cap. After the head is set into a deep cavity, the fibrous surface of the capsule adheres to it, and head movements occur inside the capsule. In children under 8 years old age, this operation gives good results.M. V. Volkov suggested using specially prepared caps, consisting of 60-70 layers of the amniotic membrane, as a gasket (see Arthroplasty).
With severe antetorsion of the femoral head, open reduction is combined with corrective osteotomy. Transverse intertrochanteric osteotomy with antetorsion correction, and if indicated, with varization, osteosynthesis with a pin or other design, has become widespread. Patients over 8 years of age undergo the Chiari operation - a horizontal osteotomy of the iliac body directly above the roof of the acetabulum. As a result of the displacement of the distal fragment of the pelvis, the proximal fragment of the ilium hangs over the head of the femur. In the presence of antetorsion of the head, the operation is supplemented with intertrochanteric osteotomy. In order to create a strong canopy over the femoral head in case of subluxation, a number of operations have been proposed, of which the main one is Salter's operation (osteotomy of the ilium body with the introduction of a triangular autograft taken from the iliac crest, or allograft, into the split).
Among palliative operations it is necessary to note operation In - Lami, to-ruyu apply as auxiliary intervention. Its principle is reduced to bringing down a part of the greater trochanter along with the middle and small gluteal muscles attached to it. The purpose of operation - to strengthen these muscles at the expense of a nek-ry their tension. The cut-off part of the greater trochanter is fixed with a screw or wire to the outer surface of the femur at the base of the greater trochanter or slightly lower. The infratrochanteric osteotomy of the femur according to Shantz, which was previously used for high iliac dislocation, is now almost never used, since it is ineffective and often leads to the development of genu valgum (see Knee joint). In adolescents and adults with unilateral congenital dislocation, in some cases, art rodesis is indicated (see) - strengthening the joint in a fixed position. At the same time, due to the forced reduction of the femoral head and its reduction into the deepened acetabulum, it is possible to lengthen the leg. The most reliable is intra-extra-articular arthrodesis with fixation of the femoral head to the roof of the acetabulum with a three-bladed nail. In addition to the nail, bone plates and more complex structures are also used for fixation. As a result of the operation, the limb's support is restored and pain in the joint is eliminated, which allows the patient to perform even hard physical work.
The forecast at patients with malformations of T. page. largely determined by the timeliness of diagnosis and treatment; in most cases, a good functional result is achieved by conservative methods. With congenital dislocation and subluxation of the hip, the detection of a defect in the first weeks and months of life allows it to be eliminated without consequences. In cases of later detection, the results of the treatment of the defect worsen; there is a need for the use of surgical intervention, a cut, however, does not provide a complete restoration of the function of the hip joint.
Damage
T.'s damages with. include bruises, traumatic dislocations of the hip, traumatic dislocations of the hip in combination with fractures of the head, neck of the femur and acetabulum, epiphysiolysis, damage to the hip joint in combat trauma.
Bruises of area T. with. may be accompanied by damage to soft tissues and joint elements, the formation of subcutaneous or intermuscular hematomas. Sometimes, especially against the background of arthrosis (see), the elements of the joint are damaged - articular cartilage, spiny outgrowths, articular capsule. This can lead to prolonged pain - co-xalgia.
In detail a wedge, a picture, diagnostics and treatment - see the table. The prognosis is usually favorable.
Traumatic hip dislocations usually occur as a result of indirect trauma. Depending on the position of the femur at the time of injury, the displacement of the head of the bone occurs in different ways. Distinguish back dislocations of a hip (the most frequent, making up to 80% of all dislocations of T. page). upward and backward - iliac dislocation (luxatio iliaca), downward and backward - sciatic dislocation (luxatio ischiadica); anterior dislocations: anteriorly and upwards - suprapubic dislocation (luxatio pubica), forward and downward - obturator dislocation (luxatio obturato-ria); with fractures of the bottom of the acetabulum - central dislocation (luxatio centralis). Clinically, hip dislocations are manifested by severe pain in the hip joint, lack of active movements, forced position of the limb, depending on the type of dislocation (see Fig. 3 to Art. Dislocations).

The diagnosis is clarified by radiography: the acetabulum is empty, and the femoral head is displaced upward, to the level of the ilium body (Fig. 11) or downward, to the level of the lower branch of the pubic bone (Fig. 12). X-ray diagnostics of back dislocation is the most difficult, for identification to-rogo examine width of a joint crack all over and the ratio of a hip to the reference points described above. X-rays in some cases reveal concomitant fractures of the neck, femoral head and acetabulum. Fracture of the femoral head, often of its lower segment, occurs at the moment when it is displaced beyond the edge of the acetabulum.

Acetabular fractures, according to L. G. Shkolnikov, V. P. Selivanov, V. M. Tsodyks (1966), account for 7.7% of the total number of pelvic fractures and are usually combined with other pelvic fractures (see). In particular, fractures of the walls of the acetabulum are usually accompanied by a dislocation of the femur (Fig. 13). The mechanism of acetabular fractures is compression of the pelvis in the frontal plane, a blow to the greater trochanter, which often occurs when falling from a height. A fracture of the upper edge of the acetabulum is easily diagnosed radiographically, while fractures of the anterior or posterior edge may be masked by the shadow of the femur and pelvic bones. Therefore, in case of joint injuries, one should not be limited to shooting in one standard projection, but supplement it with a second - semi-lateral. A fracture of the acetabular floor is often accompanied by a central dislocation of the femoral head. In this regard, two groups of acetabular fractures are distinguished: without primary displacement of the head and with its displacement and central dislocation (Fig. 14). With a central fracture-dislocation, the head of the femur, which is displaced inward, pushes through the inner wall of the acetabulum and is displaced into the pelvic cavity. At the same time, the position of the limb is forced, movements are impossible, retraction in the region of the greater trochanter is noted. Rectal examination can sometimes determine the bulging in the bottom of the acetabulum. The radiograph shows the displacement of the femoral head into the pelvic cavity, sometimes together with bone fragments of the bottom of the acetabulum.
Treatment of traumatic hip dislocation includes manual closed reduction, open reduction, sometimes in combination with other operations (arthrodesis, arthroplasty, osteosynthesis). Closed reduction of hip dislocation is most often performed using the Kocher method under anesthesia, preferably with muscle relaxants. The patient is placed on his back. The assistant holds the patient's pelvis with his hands, and the surgeon bends the injured leg in T. s. at a right angle and pulls along the thigh, rotates the thigh inward, then outward, abducts and unbends. At this moment there is a reposition (see). With difficult-to-reduce iliac dislocations, it is necessary to bring the head of the bone to the notch of the acetabulum and reduce the dislocation through it. In addition to what has been described, other ways to reduce hip dislocation have been proposed (see Dislocations). At the same time, the success of the operation depends more on good anesthesia and muscle relaxation than on the choice of reduction method. After reduction of the dislocation, immobilization is performed (see) using a coxite plaster bandage, adhesive plaster (in children) or skeletal traction of the limb with a load of 3-4 kg. Walking on crutches is allowed after 3-4 weeks; You can load the limb after 5-6 months. after injury. An earlier loading is dangerous due to the possible development of aseptic necrosis of the femoral head.
If the dislocation was accompanied by a fracture of the posterior edge of the acetabulum and the reduction turned out to be unstable due to the detachment of a large bone fragment, fixation of the fragment with screws is indicated. After that, it is advisable for 1 - 2 months. carry out skeletal traction along the length of the limb to prevent aseptic necrosis of the femoral head.
Treatment of central dislocation is carried out by skeletal traction for the condyles of the femur. If the head is not removed, skeletal traction is simultaneously carried out for the greater trochanter perpendicular to the axis of the limb for 2-3 months. If, in this case, the reduction of the femoral head fails, resort to surgical reduction of the dislocation. Full load of the limb is allowed after 6 months. after injury. In childhood, with a fracture of the acetabulum, damage to the Y-shaped cartilage is often observed, which can lead to a violation of the growth of the cavity and its inconsistency with the size of the femoral head.
Pathological dislocations in T. with. occur when the femoral head is destroyed by an inflammatory process (see Coxitis). Often it occurs with coxitis in infants due to umbilical sepsis. Pathological also include hip dislocation with residual effects of poliomyelitis. Patol. Central dislocation is observed when the bottom of the acetabulum is destroyed by a tumor. Treatment and forecast patol. dislocations depend on the nature of the underlying process.
Fracture of the femoral neck often occurs in old age. Such fractures (subcapital, intermediary). if they are not driven in, they do not grow together with conservative treatment. The main surgical method of treatment is osteosynthesis (see), and with a subcapital fracture - endoprosthesis replacement (see). In case of an ununited fracture or false joint of the femoral neck, a combined operation is used - osteosynthesis with a Smith-Petersen metal nail and McMurray intertrochanteric osteotomy. Sometimes a bone graft from a large trochanter on a muscular pedicle is brought to the area of the false joint (see Thigh).
Epiphyseolysis of the femoral head is observed in adolescents, more often in the period from 11 to 16 years. The epiphysis is usually shifted backwards and slightly downward, in some cases there is a complete displacement of it downwards. The displacement of the epiphysis is observed, in particular, with congenital coxa vara. Clinically, epiphysiolysis is manifested by lameness, limitation of movements in the T. s., slight shortening and external rotation of the limb, and limitation of internal rotation. At rentgenol. research, in addition to a direct picture, it is necessary to do a lateral radiograph, since often only a displacement of the epiphysis is detected on it. Treatment of epiphysiolysis is aimed at stopping further displacement of the epiphysis or its reduction and fixation. If the displacement is small, but there is a tendency to progression, closed osteosynthesis with wires or a nail is necessary. With a significant displacement, reposition is achieved by skeletal traction followed by osteosynthesis with a nail. In cases of chronic epiphysiolysis, an intertrochanteric osteotomy is performed to eliminate coxa vara. In the presence of epiphysiolysis on one side, X-ray control of the femoral head of the opposite side is necessary.
The prognosis for traumatic hip dislocation, especially in combination with fractures of the head, neck of the femur and acetabulum, in most patients in relation to the restoration of T.'s function. unfavorable due to the development of complications: aseptic necrosis of the femoral head, development of arthrosis, contracture.
With traumatic epiphysiolysis, arthrosis of T. often develops; this is due to the difficulty of accurate repositioning of the femoral head and a violation of the biomechanics of the joint.
Combat damage, staged healing
Closed combat injury T. s. (dislocations, intra-articular fractures) is relatively rare and does not differ significantly from similar injuries in peacetime. The main type of combat injury T. s. - bullet and shrapnel wounds. In the focus of mass destruction, injuries from secondary shells are also likely.
T.'s wounds with. are divided into non-penetrating, with damage only to soft tissues, and penetrating into the joint cavity, with or without damage to bone tissue. According to the experience of the Great Patriotic War, T.'s wounds with. accounted for 6.6% of all injuries of large joints (excluding the wrist), and almost half of them were penetrating; bone damage in penetrating wounds was observed in 93.6% of cases. Bone fractures are more extensive and complex than with a closed injury, so their division into fractures of the femoral head, its neck, fractures of the articular cavity, intertrochanteric and subtrochanteric fractures is conditional. A wounding projectile, damaging the bone, even outside the joint cavity, can cause the formation of far-reaching cracks and large fragments, while the fracture may actually be intra-articular. The destruction of the periarticular soft tissues is sometimes very extensive, especially when injured by a large fragment of metal, and bullet wounds often penetrate through the bones of the joint into the pelvic cavity.
Gunshot injury T. s. according to the severity of the damage, it ranks first among the injuries of other large joints. Simultaneously with T. s. iliac, femoral, gluteal vessels, sciatic nerve can be damaged.
The wedge, the picture with a significant destruction of the bone elements of the joint and a visible change in its shape, position and length of the thigh is typical; the diagnosis in these cases does not cause difficulties. For specification of localization and a form of damage of T. page. it is necessary rentgenol. study.
First aid (see) and first aid (see) include the imposition of an aseptic bandage, the introduction of painkillers, transport immobilization of the entire limb and torso with standard or improvised means (see Immobilization). When rendering first aid (see), the bandage is corrected, the immobilization is corrected and improved using standard splints (see Splinting), antishock liquids, antibiotics are injected. Qualified medical care (see) includes anti-shock measures, the final stop of bleeding, as well as primary surgical treatment of the wound (see) in cases where its delay is unacceptable (extensive, crushed or obviously contaminated wounds). The specialized medical care (see), rendered in to lay down. institutions of the front hospital, in traumatological hospitals of the hospital base of medical. GO services, includes primary delayed or secondary debridement and surgical intervention on the joint itself. In this case, its resection is most often indicated, since arthrotomy does not provide sufficient drainage. It is recommended to remove the head and neck of the femur, then comparing it with the sawdust of the acetabulum, fixing the limb with a high plaster cast in the position of a slight abduction.
Of the complications, the most common are wound suppuration (see Wounds, wounds), sometimes with streaks, osteomyelitis (see), anaerobic infection (see), 20% of complications are sepsis (see). Often, repeated operations are required - opening of streaks and their drainage (including in the pelvic cavity) and, in extreme cases, hip disarticulation.
The prognosis is unfavorable. The combat capability of the wounded is restored Ch. arr. after extra-articular wounds, and even then not always. According to the experience of the Great Patriotic War, with penetrating wounds, the duration of treatment in most cases was 200 days or more; almost 9% of the wounded lost a limb, and in about 50% it remained functionally disabled.
See also the table to this article.
Diseases
To inflammatory diseases of T. page. include periarthritis (see), bursitis (see), arthritis (see).
Periarthritis is called periarticular lesions associated with an infectious-allergic process, often against the background of dystrophic changes. Treatment is reduced to conducting thermal and physiotherapeutic procedures and prescribing anti-inflammatory drug therapy. The prognosis is favorable.
Bursitis in the area of T. s. sometimes takes a severe course. The synovial bursae of the greater trochanter and the iliac crest bursa are usually affected. With purulent inflammation of the latter, the process can spread to T. s. Bursitis in the region of the greater trochanter often has a tuberculous etiology (see Trochanteritis; Tuberculosis extra-pulmonary, tuberculosis of the bones and joints.). Treatment is anti-inflammatory, antibacterial; favorable outcome.
Arthritis I.e. I can be of various etiologies - tuberculous, acute purulent, rheumatic, gonorrheal, etc. (see Coxitis, as well as the table to this article).
Dystrophic diseases T. s. are very common. They are based on injuries T. page, coxitis, congenital deformities, metabolic and trophic disorders (see Arthrosis). With the ineffectiveness of their conservative treatment, surgical interventions are indicated to change the biomechanics of the joint (osteotomy, cutting off and transplantation of regional muscles, etc. To create ankylosis (see Arthrodesis), and in some cases endoprosthesis replacement (see).
Osteochondromatosis T. s. (see. Hond-romatosis of the joints) is rare. Clinically, it is manifested by periodic blocking of the joint (infringement of free osteochondromatous bodies), accompanied by a sharp sudden pain. Surgical treatment - arthrotomy and removal of free bodies. In cases of gross lesions of the articular cartilage, the same surgical methods are used as in case of arthrosis. Timely and radical removal of chondromatous bodies leads to recovery.
Aseptic necrosis of the femoral head occurs as a complication after forced reduction of congenital hip dislocation or after a fracture of the femoral neck, especially subcapital, and may also be of unknown etiology. In children, this disease has a number of clinical and morphological features and is known as Legg-Calve-Perthes disease (see Perthes disease). It is manifested by lameness, pain in T. with., radiating to the knee joint, contracture. Treatment is reduced to unloading the limb (walking on crutches), conducting physiotherapy procedures; if these measures fail, surgical treatment is indicated. In adults, osteotomy, arthrodesis, or endoprosthesis are performed, which largely restores T.'s function.
To diseases of T. page. also include acquired forms of coxa vara, resulting from rickets, osteomyelitis of the femoral neck, trauma to the proximal end of the femur.
Tumors T. with. may come from the joint capsule (see Synovioma). from cartilage and bone tissue. In the neck of the femur, benign tumors are observed - osteoma (see), osteoid osteoma (see), osteoblastoclastoma (see), chondroma (see), chondroblastoma (see), as well as malignant tumors - chondrosarcoma (see .), osteogenic sarcoma (see).
Treatment of benign tumors usually involves their excochleation (curettage) or resection of the affected bone within healthy tissues. It is advisable to fill the postoperative defect with bone auto- or allografts. In malignant tumors, extended resection of the proximal end of the femur is indicated, followed by replacement of the resected area with a bone allograft or endoprosthesis. In advanced cases, exarticulation of the thigh or interilio-abdominal amputation is performed. Radiation and chemotherapy are used according to indications.
The prognosis for benign tumors is favorable, but in the future, the development of deforming arthrosis of T. is possible. At malignant tumors the forecast is defined gistol. tumor form and timeliness of treatment.
Clinical and diagnostic characteristics and methods of treatment of major malformations, injuries, diseases and tumors of T. page - see the table.
OPERATIONS
Operative interventions on T. page. produce with destructive processes in the joint itself and near it, with tumors, dystrophic diseases, congenital and acquired deformities, etc. They are characterized by a relatively high degree of trauma, therefore anesthesia is preferable as an effective means of anesthesia in most cases (see); use also spinal, epidural and local anesthesia (see).
Operational accesses to T. page. numerous. A variety of pathology, complexity of anatomy of area T. page. requires a differentiated approach to the choice of access. Anterior approaches are indicated for operations on the head and neck of the femur; the most used are accesses according to Jaeger - Textor, Guther, Lyukka - Shede, Gharibdzhanyan (see Koksit). External accesses include operational approaches according to White, Spren-gel, Hagen-Thorn, Shassenyak (see Koksit). With their help, exposure of the distal femoral neck and posterior lower ilium (posterior acetabular lesions) is achieved. More traumatic access according to Ollie - Lexer - Murphy - Vreden, consisting in an arcuate (curvature downwards) dissection of the skin under the greater trochanter, cutting off the latter and turning the musculocutaneous flap upwards. This achieves a wide view of the entire joint.
The most common posterior approaches are the Kocher and Langenbeck approaches, with which the gluteus maximus is stratified along the fibers, and the joint is opened from behind. These accesses are most indicated for drainage arthrotomies (see) with purulent coxitis.
Operations on T. page. can be divided with a certain conventionality into diagnostic, corrective, radical, palliative. Diagnostics include a puncture to extract intra-articular fluid or a biopsy of the tissues of the joint. The puncture is made in front, outside and behind.
Arthrotomy T. s. use for an exposure of a joint as operational access or with to lay down. purpose (eg, to drain a joint).
Resection of T. page. shown in destructive processes and tumors. This operation consists in the removal of pathologically altered tissues within a healthy bone and, along with the rehabilitation of the joint, its ankylosing aims.
Osteotomy of the trochanteric region of the thigh is most often performed to eliminate the vicious position of the limb with T.'s contracture, arthrosis, and aseptic necrosis of the femoral head. For the last two indications, a McMurray osteotomy is usually performed; a longitudinal incision is made from the top of the greater trochanter downwards 12-15 cm long, the muscles are subperiosteally separated from the trochanteric region; a chisel produces an oblique osteotomy and, retracting the thigh, the proximal fragment is displaced medially under the neck and head of the femur. The operation is completed by applying a plaster cast. The result of this operation is a change in the load on the femoral head, as well as stimulation of reparative processes in its head and neck.
In some cases, osteotomy (see) is palliative, for example, osteotomy according to Shants - trochanteric fa-naya osteotomy with emphasis on the proximal fragment in the ischium.
Arthrodesis T. s. varied. Intra-articular arthrodesis is similar in technique to resection. In some cases, it is supplemented by the introduction of bone grafts between the femoral head and the acetabulum or fixation of the head in the cavity with metal fixators (pins, screws, compression devices). In Vreden arthrodesis, the role of the fixator is performed by a long bone graft passed through the neck, head, and acetabulum. Extra-articular arthrodesis involves the immobilization of the joint without opening it, for example, with the help of a bone autograft between the greater trochanter and the ilium. Arthrodesis (see) has an end goal ankylosis of the joint, but does not provide for direct intervention on patol. hearth, therefore, in most cases, it belongs to the category of palliative operations. In a crust, time arthrodesis is used less and less.
Arthroplasty (see) - various interventions that provide for the mobilization of T. s., the restoration of its mobility; can be performed using auto- and allografts.
Endoprosthetics (see) is widely used. Various models of metal, metal-polymer and ceramic endoprostheses are used, which allow restoring mobility in T. s. with its destruction or after extensive resections for tumors.
With malformations of T. page, in addition to corrective osteotomies of the femur, reconstructive operations on the acetabulum, aimed at deepening it (Salter's, Chiari's operations, etc.), have become widespread; in congenital dislocation of the hip in children under 8 years of age, capsular arthroplasty is successfully used (Codiville's operation - Columns and its modifications). Operation of the Column is offered for restoration of mobility of T. page. in case of destruction of the femoral head: instead of the head, a severed greater trochanter is introduced into the acetabulum. Operation is ineffective and in a crust, time is applied seldom.
Conducting patients after operations on a hip joint includes the general actions (see the Postoperative period), and also an immobilization of a joint for various terms depending on character patol. process and operation. Drainage of the joint is mandatory to prevent the formation of a hematoma. With prolonged immobilization, much attention is paid to the prevention of congestion in the lungs, vascular disorders, bedsores.
Table. CLINICAL AND DIAGNOSTIC CHARACTERISTICS AND METHODS OF TREATMENT OF MAJOR DEVELOPMENTAL DEFECTS, INJURIES, DISEASES AND TUMORS OF THE HIP JOINT
|
The name of the malformation, injury, disease, tumor (typed in italics is published in separate articles) |
Main clinical manifestations |
Data from special research methods (X-ray, laboratory, histological, etc.) |
Treatment Methods |
|
Malformations |
|||
|
Congenital coxa vara |
Wide leg stance (P-position), "duck" gait, positive Trendelenburg-Duchenne sign; adduction and external rotation of the hip is determined, internal rotation and abduction of the hip are limited; Bryant's triangle is broken, the greater trochanter is located above the Roser-Nelaton line, the Shemaker line is displaced |
X-ray. examination ■ - on the survey radiograph - an increase in the acetabulum, the size of the greater trochanter, the epiphyseal growth zone is located vertically, expanded, the cervical-diaphyseal angle is reduced |
Conservative methods (effective only with early diagnosis): massage of the muscles of the thigh and pelvis, prolonged bed rest with traction for the thigh; to lay down. gymnastics; preparations of calcium, phosphorus and general anti-rachitic therapy in combination with physiotherapy and dignity. - chickens. treatment. Surgical treatment in children over 12 years of age and in adults is reduced to the reconstruction of the proximal femur in order to eliminate the vicious position of its head and neck using various osteotomy methods. |
|
Congenital plow valga |
Restricted hip abduction, positive Trendelenburg-Duchenne sign, no signs of hip dislocation, limb lengthening, low standing of the greater trochanter |
X-ray. study - an increase in the cervical-diaphyseal angle, the epiphyseal growth zone approaches the horizontal line, pronounced antetorsion, underdevelopment of the acetabulum, displacement of the femoral head proximally (without dislocation) |
With functional disorders caused by decentration of the femoral head, various options for varus osteotomy are indicated. |
|
Congenital dislocation of the hip |
Limitation of abduction and internal rotation of the thigh, shortening of the leg, positive Trendelenburg-Duchenne symptom, asymmetry of skin folds on the thighs, the greater trochanter is displaced upward and is located above the Roser-Nelaton line, the Shemaker line is displaced, a positive Marx symptom is noted, flexion contracture of the hip joint, muscle hypotrophy on the side of dislocation, pelvic tilt and scoliotic posture, with bilateral dislocation - "duck" gait and pronounced lumbar lordosis |
X-ray. examination - signs of hip dysplasia, antetorsion of the femoral neck, location of the head outside the acetabulum, confirmed by arthrography |
Conservative treatment (indicated for reducible dislocations): dilution of the hips with the help of pillows and spreading splints, to lay down. gymnastics, massage of the gluteal muscles and thigh muscles. Surgical treatment (when closed reduction of dislocation is impossible) includes operations on the acetabulum and the proximal end of the femur: open reduction of the femoral head, deepening of the acetabulum using an amniotic cap, Salter, Chiari operations, resection of the femur to bring its head down, some rye palliative operations, as well as art rodez; in some cases, these operations are combined with preliminary skeletal traction, which contributes to the reduction of the femoral head |
|
Congenital subluxation of the hip |
Clinical signs are the same as in congenital hip dislocation, but less pronounced |
X-ray. research - signs of hip dysplasia are determined, the femoral head is partially located in the acetabulum. Arthrography reveals inadequate coverage of the femoral head by the roof of the acetabulum |
Conservative treatment is the same as for congenital hip dislocation. Surgical treatment is the same as for congenital dislocation of the hip, but the bringing down of the femoral head is excluded. |
|
hip dysplasia |
Limitation of abduction and internal rotation of the hip, possibly combined with other malformations of the musculoskeletal system |
X-ray. research - on the survey radiograph of the hip joints, various degrees of smoothing of the acetabulum, underdevelopment of bone structures, an increase in the size of the femoral head and its inconsistency with the entrance to the acetabulum are determined, however, there is no data confirming dislocation or subluxation of the hip. On axial images - valgus or varus position of the proximal end of the femur, antetorsion of its neck |
Conservative treatment: various ways of spreading the legs with the help of pads between the legs of the child; spreading tires Volkov, Vilensky; functional treatment - crawling with legs apart. Surgical treatment: operations aimed at deepening the acetabulum, mainly by creating its “roof” (Salter, Chiari operations and their modifications), operations at the proximal end of the femur to eliminate antetorsion, valgus and varus deformity of the neck (osteotomy) |
|
Damage |
|||
|
Closed damage |
|||
|
Traumatic hip dislocation |
1 Severe pain in the hip joint, when combined with [other injuries, traumatic shock is possible, active |
X-ray. study ■ - the absence of the femoral head in the acetabulum, it is projected above, below or medially |
Under anesthesia, a closed manual reduction of the dislocation is performed, followed by radiography; after reduction, coxite plaster is applied |
|
nye movements in the joint are impossible, when trying to passive movements - springy resistance; forced fixed position of the lower limb: with iliac (posterior superior) dislocation, the leg is slightly bent, adducted and rotated inward, shortened; with ischial (posterior inferior) - sharply bent at the hip joint, adducted and rotated inward, shortened; , slightly abducted and rotated outward, shortened, with obturator dislocation (head at the obturator foramen of the pelvis) the leg is bent, abducted and rotated outward, not shortened; with central dislocation - the impossibility of active and passive movements, unsharp external rotation, shortening of the leg |
but from the acetabulum; with a concomitant fracture of the femoral head, a lunate shadow of a fragment of its upper or lower pole is visible. In case of dislocation of the hip in combination with a fracture of the edge of the acetabulum, a sickle-shaped, crescentic or beak-shaped shadow of the fragment is visible on the radiograph. The fracture of the acetabulum is contoured as a gap with jagged edges, the femoral head is displaced medially, sometimes into the gap of the fracture of the cavity, Shenton's line is broken. A fracture of the acetabulum is often accompanied by a fracture of the ilium, ischium, and pubis. With cystography with tight filling of the bladder, the shadow of the bladder is displaced to the opposite side of the fracture by a retroperitoneal hematoma formed around the acetabulum |
bandage or skeletal traction for 3-4 weeks, then allowed to walk on crutches without load on the leg for 5-6 months; prescribe thermal baths, massage of the muscles of the pelvic girdle, exercise therapy, swimming. In case of dislocation fractures, fragments of the femoral head are removed, open reduction, arthrodesis or endoprosthetics are performed, depending on the degree of damage to the head; a fragment of the posterior edge of the acetabulum is subject to open reduction and fixation with screws. In case of fractures of the acetabulum and central dislocation of the hip, skeletal traction is performed with a load of 8–10 kg for the epicondyle of the femur on the Beler splint or bed plane with hip abduction for 2–3 months; in the absence of reduction (X-ray control after 3-4 days) - additional traction for the region of the greater trochanter. At the same time, massage, electrical muscle stimulation are prescribed, after removal of traction - exercise therapy, massage, warm baths, swimming, walking on crutches without load on the leg for 6 months. With a significant displacement of the fragments of the bottom of the acetabulum and the absence of reduction during skeletal traction, an open reduction of fragments of the acetabulum and their fixation with a plate or screws is shown |
|
|
Hip injury |
Pain when walking with maintaining leg support. The position of the leg is normal, active movements in the joint are limited and painful, sometimes a subcutaneous hematoma bulges in the region of the greater trochanter. |
X-ray. examination - bone damage is not determined |
Bed rest for 7-10 days, on the 3rd-4th day after the injury - warm baths, UHF on the area of T. s. |
|
Epiphysiolysis of the femoral head |
The leg is fixed in the position of external rotation, shortened, movements in the joint are limited, especially internal rotation; lameness, atrophy of the gluteal and femoral muscles are noted |
X-ray. research - on radiographs in the anteroposterior and lateral projections, the varus displacement of the femoral head along the line of the growth cartilage of the epiphysis is determined |
With a significant displacement of the femoral head - skeletal traction; after removal of the displacement or with a non-sharp displacement - osteosynthesis with knitting needles or a pin |
|
Open damage |
|||
|
Wounds (shrapnel, bullet, bayonet, knife, etc.) Non-penetrating wounds |
Entrance openings (single or multiple) are more often located in the gluteal region, bleed; wound channels (single or multiple) usually pass above or below the femoral neck, contain foreign bodies, scraps of clothing, destroyed muscle layers, blood clots; movements in the joint with single wounds are not impaired, with multiple wounds they are limited |
X-ray. study - changes may be absent; para-articular sometimes metal foreign bodies are determined |
With single stab wounds, primary surgical treatment is not indicated; in other cases, the tissues are dissected, infiltrated with a solution of antibiotics, an aseptic bandage is applied, the joint is immobilized |
|
Penetrating wounds without damage to the bones of the joint |
Wound channel - single or multiple, inlet and outlet can be the same as in non-penetrating wounds, but differ in a more complex location in the tissues around the joint; often in the inlet, areas of the damaged joint capsule are visible, the outflow of synovial fluid is practically not observed; movement in the joint is limited and painful |
X-ray. research - sometimes expansion of the joint space, thickening of the joint capsule and pneumoarthritis; foreign bodies may be found around the joint, as well as fractures of other bones |
Surgical treatment is carried out in two stages: in the early stages - wide dissection and excision of tissues, especially the gluteal muscles, their infiltration with antibiotics, application of an aseptic dressing, immobilization; in the later stages - according to the testimony of arthrotomy; with infectious complications of the wound - opening of purulent streaks; after surgery, immobilization of the hip joint is mandatory |
|
Penetrating wounds with damage to the bones of the joint |
Often, especially with combined injuries, a picture of traumatic shock develops; extensive destruction of the soft tissues of the gluteal region (inlet), the presence of free bone fragments in the wound canal, crushing of the acetabulum, head and neck of the femur lead to significant blood loss, aggravating the severity of shock; limb in a forced position, shortened; active movements in the joint are impossible, passive ones are sharply painful |
X-ray. the changes are varied: multi-comminuted fractures of the neck, the head of the femur with their displacement in various directions, extensive destruction of the acetabulum, perforated injuries of the bones of the joint, single and numerous foreign bodies in the tissues around the joint and in the bones; sometimes a sharp displacement of the femoral head with its complete dislocation from the acetabulum; possible combination with damage to other bones. Localization and depth of foreign bodies in the bones are detected using tomography |
Anti-shock measures: analgesics, injection of 1-2% solution of novocaine into the area of bone damage, bandaging, immobilization, blood transfusion. Primary surgical treatment (indicated for the vast majority of penetrating wounds of the joint): dissection and excision of soft tissues, removal of loose bone fragments and visible foreign bodies, tissue infiltration with antibiotic solutions. At the stages of qualified and specialized medical care, according to strict indications, early primary resection of the bone is acceptable, according to vital indications, disarticulation of the limb. After surgical treatment, a plaster cast is applied |
|
Diseases |
|||
|
brucellosis |
Periodic pain without a pronounced dysfunction of the joint. In rare cases, a rapid course with severe pain, with a significant amount of effusion in the joint, fever and a sharp increase in local temperature; characterized by inflammation of the mucous bags; often accompanied by sacroiliitis of the same etiology. In untreated cases, spontaneous ankylosing is possible, sometimes in a vicious position |
X-ray. research - osteoporosis, usuration of articular surfaces, in the later stages - narrowing of the joint space, bone proliferates. The study of joint fluid is not very specific. Serological tests of Wright and Huddleson, Burne's test, Coombs' test, etc. are positive |
Treatment of the underlying disease; locally: massage, mud applications, to lay down. physical education aimed at preventing muscle atrophy and maintaining joint mobility, physiotherapy, radon baths |
|
Gonorrheal |
The onset is acute on the 2nd - 3rd week of gonorrhea: severe pain in the joint, fever, local fever, flexion-adductor contracture. The mobility of the joint decreases rapidly, until the onset of ankylosis |
X-ray. research - rapidly progressive narrowing of the joint space, uneven fuzzy contours of the articular ends of the bones and their pronounced osteoporosis. Bone ankylosis is formed early. Gonococcus is cultured from the synovial fluid |
Treatment of the local process is carried out against the background of general therapy: antibiotics are injected into the joint, in the active stage, immobilization in a functionally advantageous position is required in case of ankylosis of the joint. When ankylosis is formed in a vicious position - corrective operations (subject to a persistent remission of the process) |
|
Acute purulent |
The onset is stormy, acute, with high fever and severe pain in the joint; flexion-adductor contracture quickly appears, bone ankylosis in a vicious position is possible; characteristic abscesses, fistulas with copious purulent discharge |
X-ray. research - rapidly progressive narrowing of the joint space up to ankylosis, vicious installation of the joint; in the initial stage, osteoporosis is detected, later - osteosclerosis; the contours of the bones are uneven, in the active stage - fuzzy; in the bones of the pelvis or at the proximal end of the femur, irregularly shaped foci of various sizes are determined. Without treatment, complete destruction of the head and neck of the femur occurs, patol. upward dislocation of the hip. Wedge, blood test - changes characteristic of osteomyelitis and other purulent processes. The causative agent of the disease is isolated from the joint fluid and its sensitivity to antibacterial agents is determined. |
Immobilization of the joint, intensive antibiotic therapy. When pus appears in the joint cavity, punctures or arthrotomy are performed with drainage and constant washing with antibacterial agents. With the ineffectiveness of these measures, resection of the joint is indicated. In the case of a vicious installation of the joint (subject to a persistent remission of the process) - corrective operations |
|
With Bechterew's disease |
Unilateral lesion is rare, bilateral coxitis is more common in combination with other signs of Bechterew's disease (sacroileitis, calcification of the spinal ligaments). Manifested by persistent pain in the hip joint with irradiation to the inguinal region and downward towards the knee joint, increasing stiffness, the formation of a vicious installation of the lower extremities of the type |
X-ray. research at an early stage - osteoporosis, then narrowing of the joint space, marginal usuration; in the late stage - bone ankylosis. Rheumatoid factor in the blood is not detected. Gistol. study of T.'s tissue obtained by biopsy - proliferation of covering cells, plasmacytic and lymphohistiocytic infiltration around the vessels |
Joint unloading - walking with support on a stick, crutches; to lay down. physical education in combination with anti-inflammatory drugs such as indomethacin; san.-hens. treatment in Pyatigorsk, Tskhaltubo. With a significant decrease in the function of the joint and pronounced pain in it - arthroplasty |
|
flexion-adductor contracture, less often - flexion-abductor. Outcome - fibrous and bone ankylosis |
|||
|
For rheumatoid arthritis |
As a rule, coxitis is bilateral. Characterized by pain in the inguinal region, to-rye can irradiate along the anterior and inner surface of the thigh in the direction of the knee joint, at the same time there is a restriction of all types of movements in the affected joint. With a progressive course, flexion and flexion-adductor contractures are often formed, less often - abducting; in advanced cases, fibrous and bone ankylosis is formed |
X-ray. research - in the early phase, osteoporosis is determined, with progression - increased osteoporosis, narrowing of the joint space, usuration, sometimes protrusion of the head into the pelvis; frequent osteonecrosis, severe deformity of the femoral head up to its complete resorption and subluxation or dislocation of the hip; in some cases - fibrous and bone ankylosis. Rheumatoid factor is determined in the blood and joint fluid. The synovial fluid is turbid, sometimes bloody, the number of leukocytes is 5-10 thousand per 1 μl, with a neutrophilic shift; phagocytes are detected |
Treatment of the underlying disease. Unloading the hip joint - walking with support on a stick, crutches. With the progression of the process - synovectomy (without dislocation of the femoral head), especially with juvenile rheumatoid coxitis. Endoprosthetics is indicated in cases of a sharp decrease in the function of the hip joint |
|
Syphilitic |
It is observed in secondary and tertiary syphilis. Wedge, the picture is poor: flaccid synovitis without pain with normal function of the joint and slight effusion in it. With secondary syphilis, in parallel with skin rashes, pain in the joints (polyarthralgia), an increase in the hip joint, pronounced synovitis, flexion-adductor contracture, and atrophy of the thigh muscles are possible. With gummous syphilis, coxitis occurs in the form of synovial and bone forms. A wedge, manifestations are insignificant: periodically arising weak pains in a joint and easy lameness. Joint function is slightly impaired or not impaired |
X-ray. research - in the case of a long course, osteoporosis and bone atrophy are determined; with gummy coxitis against the background of osteoporosis, bone defects are visible - round or oval, located subchondral in the femoral head. As the process subsides, osteosclerosis increases. Positive serological tests of Kahn, Wasserman, immobilization reaction of pale treponema, immunofluorescence reaction |
The specific treatment of the underlying disease is carried out according to the appropriate scheme, at the same time physiotherapy, massage, to lay down. physical Culture. Perform corrective surgery as indicated |
|
tuberculous |
Prearthritic phase a. Minor pains in the area of the affected joint, but without a clear localization, arise and stop for no apparent reason; increased fatigue, a feeling of discomfort in the affected limb; general symptoms of initial tuberculosis. |
prearthritic phase. X-ray. research - osteoporosis in the form of a focus of enlightenment with a size of 0.5 -1.5 cm, round or oval in shape with even fuzzy edges; localization of the focus - the neck of the femur, less often - the head, pelvic bones; sometimes the centers contain small "soft" sequesters; possible narrowing of the joint space, mainly at the location of the focus. |
prearthritic phase. Immobilization of the affected joint with a plaster cast, * soft tissue traction (in children), bed rest; to delimit the process - extra- and intra-articular necrectomy with subsequent development of movements in the joint (early movements without load on the joint). Postoperative defects are filled with bone auto- or allografts. |
|
Arthritis phase. Against the background of the growing general symptoms of tuberculosis, a sudden sharp increase in pain in the joint, their clear localization; flexion-adductor pain contracture of the hip joint; atrophy of the thigh muscles, smoothness of the gluteal fold, a positive symptom of Alexandrov; patol is possible. hip dislocation upward; the joint is enlarged, which is especially noticeable against the background of soft tissue atrophy; subcutaneous abscesses, fistulas with gray-green purulent odorless discharge may appear on the thigh; palpation and movements in the joint are sharply painful. Post-starter phase. Against the background of subsiding general symptoms of tuberculosis, the perverse setting of the sustaya |
Arthritis phase. X-ray. research - a sharp narrowing of the joint space, the contours of the bones of the joint are uneven, fuzzy; regional osteoporosis of the proximal end of the femur and pelvic bones on the side of the lesion; foci of destruction against the background of general osteoporosis are poorly differentiated; bone atrophy, especially the femur. These symptoms are rapidly growing. Without treatment, relatively rapid destruction of the head and neck of the femur is possible, leading to dislocation of the hip upward. Sometimes shadows of abscesses, especially intrapelvic ones, are visible in the soft tissues. In the presence of fistulas, fistulography is obligatory, which reveals the source of the fistula and all its streaks and branches. In the absence of fistulas, but a clinically determined abscess, its puncture with aspiration is indicated |
Arthritis phase. Immobilization with a plaster cast, intensive antibiotic therapy until the intoxication is removed and the process is compensated, the destructive focus is delimited, after which extra-articular and intra-articular necrectomy, economical and reconstructive resections of the joint, etc. are performed. Post-starter phase. At the stage of the process fading, corrective operations are performed, modeling, economical, reconstructive resections, arthrolysis, bone grafting, etc. In case of exacerbation - anti-relapse treatment. In all phases in the presence of an active process - antibiotic therapy, physiotherapy, to lay down. physical education aimed at preventing muscle atrophy and joint dysfunction, heliotherapy, aerotherapy, vitamin therapy, high-calorie diet |
|
|
diductive contracture with pathological dislocation of the hip upwards, shortening of the limb with limitation of movements); bone ankylosis is rare; on the skin of the thigh and more distal limbs - post-fistulous scars; periodic exacerbations of the process are possible with a repetition of the picture of the arthritic phase; with pronounced contractures of the hip joint and shortening of the hip, secondary deformities of the pelvis, spine, and knee joint appear and gradually increase on the side of the lesion |
pus and the introduction of a contrast agent, followed by abscessography. Imaging of the joint reveals small lesions. When sowing pus and isolating the pathogen, its sensitivity to antibacterial agents is determined. Post-starter phase. X-ray. there are no signs of an active tuberculous process; the consequences of the transferred process are found in the form of gross deformities of the joint, pelvis, spine, bone atrophy on the affected side; the head and neck of the femur are often absent, there is patol. hip dislocation upward; in soft tissues shadows of abscesses and small sequesters are possible; in the bones of the joint - clear delimited foci of destruction. |
||
|
Bone-forming tumors |
|||
|
benign |
Slowly growing tumor with poor wedge, manifestations; accompanied by minor pain |
X-ray. research - a bone formation located in the neck of the femur, having a healthy bone structure or with slight osteosclerosis; localized on the surface of the bone or in its thickness |
Treatment operational - a resection within a healthy bone with removal patol. site |
|
Osteoid osteoma |
The strong accruing pains, mainly night, are precisely localized in the location patol are characteristic. hearth |
X-ray. research - against the background of the expressed osteosclerosis the center of destruction to dia is defined. up to 1 cm - so-called. tumor nest |
Surgical treatment - resection within a healthy bone. With non-radical removal, relapses are frequent |
|
Malignant tumors Osteogenic sarcoma |
Rapidly increasing constant pain, especially at night (analgesics are not very effective); the joint is enlarged, soft tissues are edematous, a pronounced venous pattern on the skin; movements in the joint are sharply painful. The tumor metastasizes early and grows rapidly. |
X-ray. research: two types of a tumor are revealed - osteolytic and osteoplastic. In the osteolytic form of sarcoma, a pronounced destruction of the bone without clear boundaries is determined, an early breakthrough of the cortical plate with the formation of the so-called. visor and needle periostitis; in the osteoplastic form of sarcoma, areas of bone formation are visible in the thickness of the tumor; tumor boundaries are indistinct. Gistol. research - cellular polymorphism, proliferation of bone tissue elements, atypical osteoid and bone structures. Wedge, blood test - anemia, accelerated ROE; increased content of mucoproteins, alkaline phosphatase |
Treatment operational; radiotherapy and chemotherapy as indicated |
|
Cartilaginous tumors |
|||
|
benign hond rob lastoma |
Gradually increasing pain, not reaching significant strength, gradual limitation of joint mobility, soft tissue atrophy |
X-ray. study - a focus of destruction in the proximal end of the femur with clear edges, containing small dotted inclusions. Gistol. research - cartilaginous tissue, consisting of chondroblasts and chondrocytes; often multinucleated giant cells |
Surgical treatment - resection of the affected area of the bone followed by bone autoplasty or alloplasty |
|
Chondroma |
The course is long, asymptomatic; possible patol. fractures; minor pain |
X-ray. research - the focus of enlightenment in the metaepiphyseal department; characteristic mottled pattern of the tumor |
Surgical treatment - resection of the affected area of the bone with subsequent bone grafting |
|
Malignant tumors Chondrosarcoma |
Rapidly increasing night pains, very strong with the central location of the tumor, less intense - with an eccentric location; joint enlargement; enhanced venous pattern on the skin; amyotrophy; painful movements, lameness. The course is relatively long |
X-ray. the study - a homogeneous focus of irregular shape with a lesion more often than the metadiaphyseal part of the bone; the cortical plate is thinned, its breakthroughs are possible. Gistol. study - tumor cartilage cells of varying degrees of atypism and polymorphism. High levels of oxyproline in the urine |
Surgical treatment: in the early stages - resection of the affected joint with bone alloplasty or endoprosthesis replacement; in later stages - disarticulation |
Bibliography: Bichem W. P. et al. Clinical study of the joints, trans. from English, M., 1970; Vilensky V. Ya. Diagnosis and functional treatment of congenital hip dislocation, M., 1971, bibliogr.; Volkov M. V. Diagnosis and treatment of congenital hip dislocation in children, M., 1969; Volkov M. V., Ter-E g and a z and r island in G. M. and Yu to and N and G. P. Congenital dislocation of the hip, M., 1972; About l at D. M. and Bron about in and c to and I am G. M. Development of a coxofemoral joint and its innervation at the person, Arkh. anat., hist. and embryol., t. 80, no. 5, p. 47, 1981, bibliogr.; Gratsiansky V. P. X-ray diagnostics of varus deformities of the femoral neck, M., 1958, bibliogr.; Zahradnichek Ya. Conservative and surgical treatment of congenital hip dislocation, Trudy Yubil. scientific session, dedicated. To the 100th anniversary of the birth of G.I. Turner, p. 137, L., 1959; Zedgenidze G. A. and Zharkov P. L. Methods of X-ray and radiological examination of the spine of large joints, Tashkent, 1979; Kaplan A. V. Damage to bones and joints, M., 1979; Kornev P. G. Surgery of osteoarticular tuberculosis, JI., 1971; Hook A. S. Varus deformity of the neck of the femur, Minsk, 1970; Lag at N about in and I. G. X-ray anatomy of a skeleton, page. 304, M., 1981; Maykova-Stroganova V. S. and Rokhlin D. G. Bones and joints in the X-ray image, Extremities, L., 1957; Marks V. O. Orthopedic diagnostics, Minsk, 1978; M about in sh about in and p I. A. and Mitrofanova A. V. Asymmetry of growth of bones of a basin at congenital dislocation of a hip and its disappearance after operational treatment, Proceedings of the 2nd All-Union. congress traumatol.-orthop., p. 308, M., 1970; The experience of Soviet medicine in the Great Patriotic War of 1941-1945, vol. 17, p. 242, M., 1953; Reinberg S. A. X-ray diagnostics of diseases of bones and joints, book. 1-2, M., 1964; Chak-l and V. D N. Fundamentals of operational orthopedics and traumatology, M., 1964; Shkolnikov L. G., Selivanov V. P. itzodyks V. M. Damage to the pelvis and pelvic organs, M., 1966; Bedouel-1 e J. Le development du cotyle normal, Rev. Chir. orthop., t. 40, p. 526, 1954; Chapchal G. Zur operativen Behandlung der dysplastischen Hiiftpfan-ne, Beitr. Orthop. Traum., Bd 24, p. 279, 1977; C h i a r i K. Geschichte und aktuelle Indikation der pfannenbildenden Eingriffe am Hiiftgelenk, Arch, orthop. Unfall.-Chir., Bd 86, S. 67, 1976; Colon-n a P. C. Capsular arthroplasty for congenital dislocation of hip, J. Bone Jt Surg., y. 35-A, p. 179, 1953; D e g a W. Osteotomia trans-ilikalna w leszeniu wrodzonej dysplazji bliodra, Chir. Narz^d. Ruchu, t. 39, s. 601, 1974; Hagymasi S. Die funktionelle Veranderung des Ligamentum acetabuliforme, dem Lebensalter und der Beanspruchung entsprechend, Acta morph. Acad. sci. hung., Bd 7, S. 249, 1957; H i p p E. Die Gefasse des Huftkopft "S, Anatomie, Angiographie und Klinik, Z. Orthop., Bd 96, S. 378, 1962; Pemberton P. A. Pericapsular osteotomy of the ilium for the treatment of congenitally dislocated hips, Clin. Orthop. , v. 98, p. 41, 1974; Salter R. B. Innominate osteotomy in the treatment of congenital dislocation and subluxation of the hip, J. Bone Jt Surg., v. 43-B, p. 518, 1961; Weber B. G. a. C e c h O. Pseudarthrosen, Bern a. o., 1973.
I. A. Movshovich; P. L. Zharkov (rents.), S. A. Rusanov (military), JI. K. Semenova (an.); tabular compilers. V. V. Gusev, M. A. Korendyasev, E. R. Mattis, V. P. Pavlov, V. F. Pozharisky.
